Downloaded 766 times



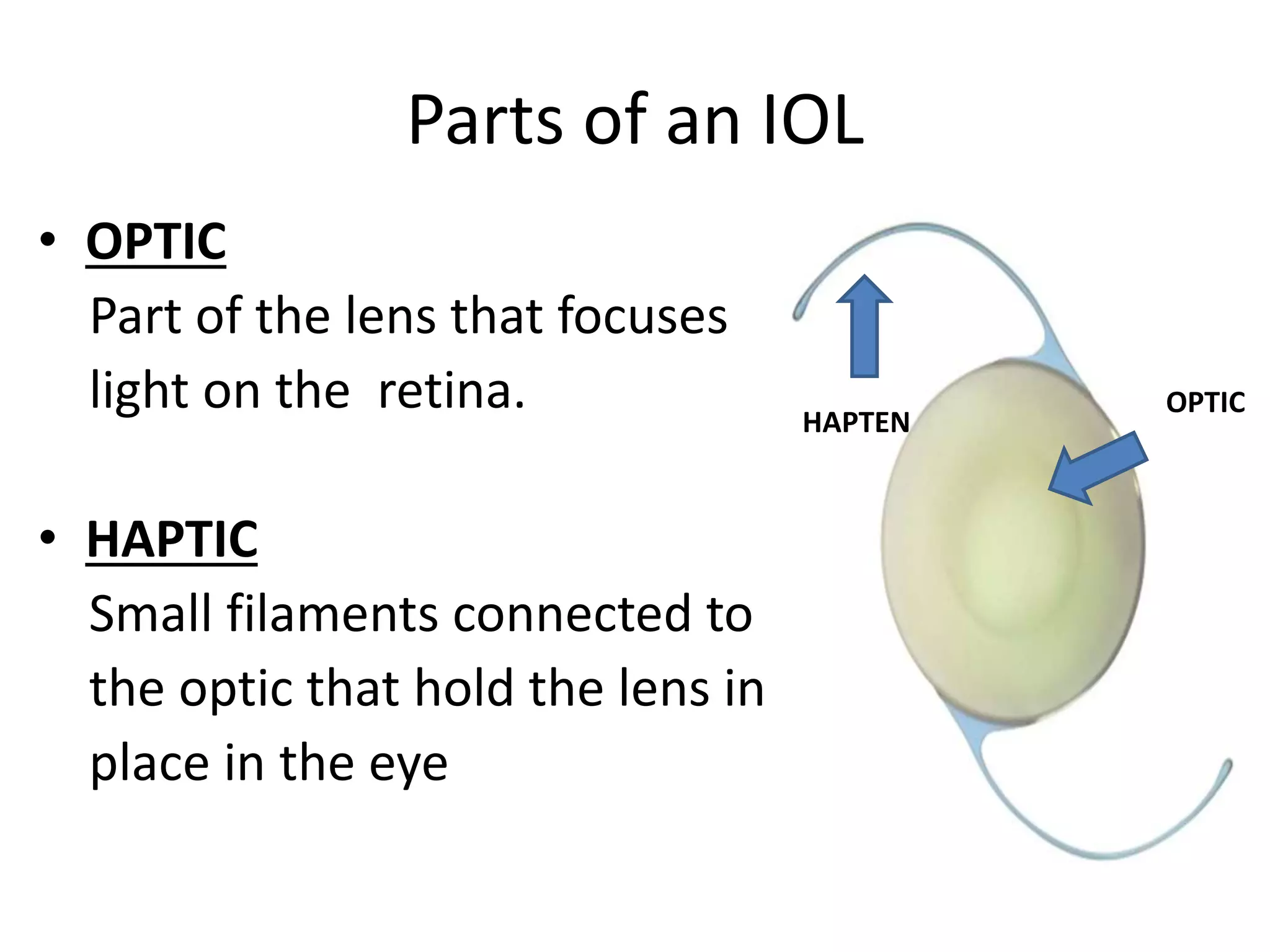
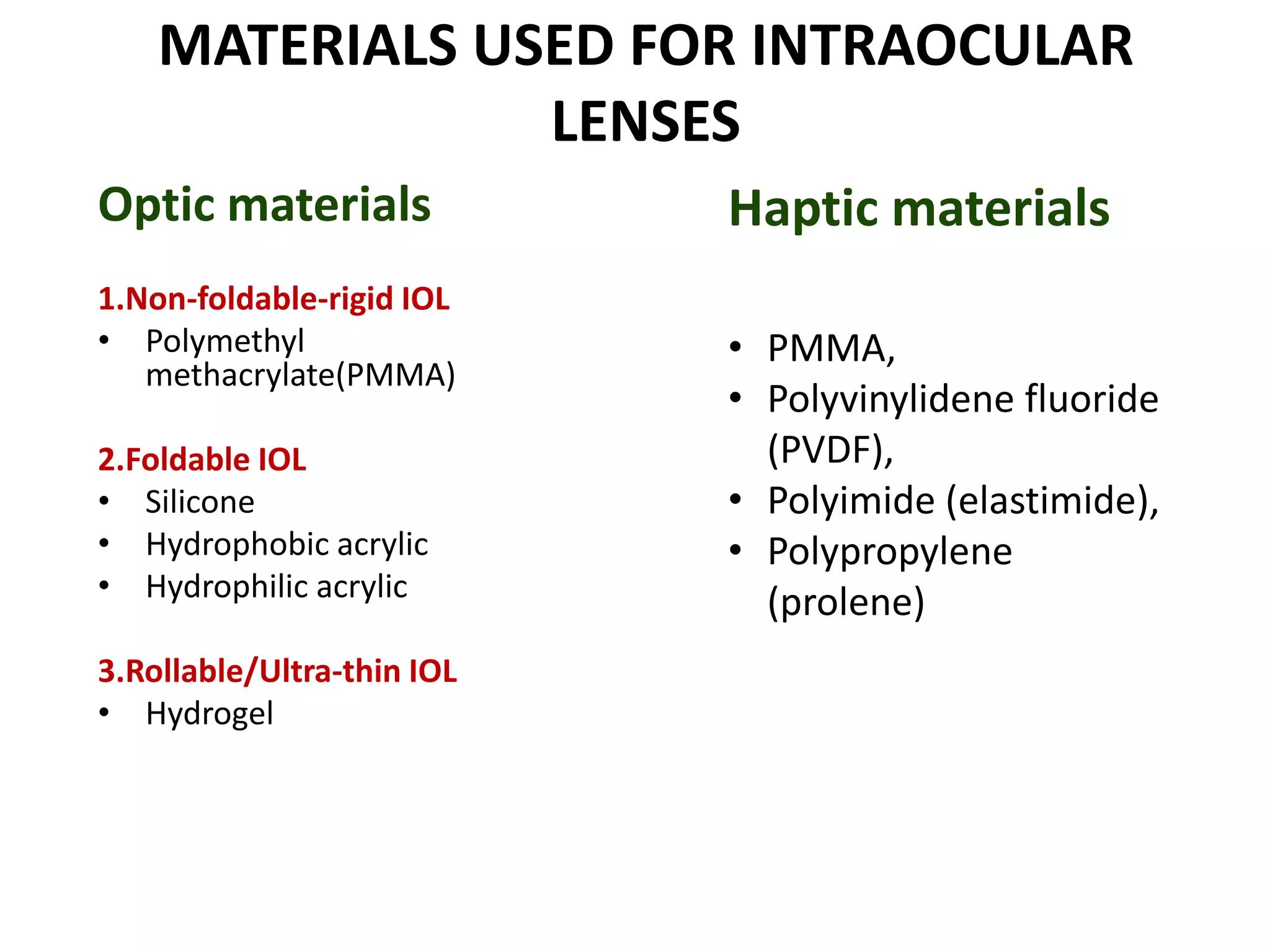

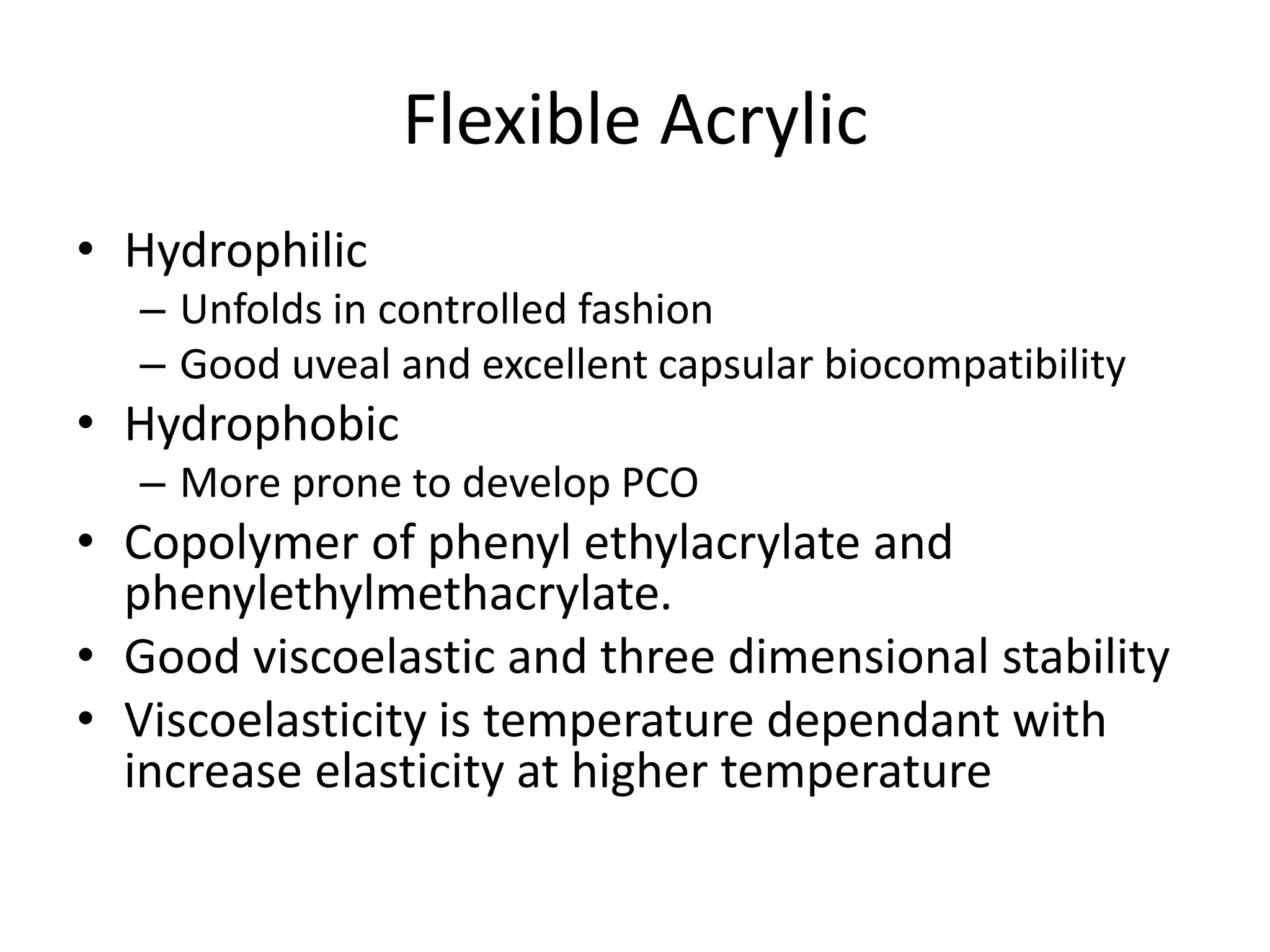














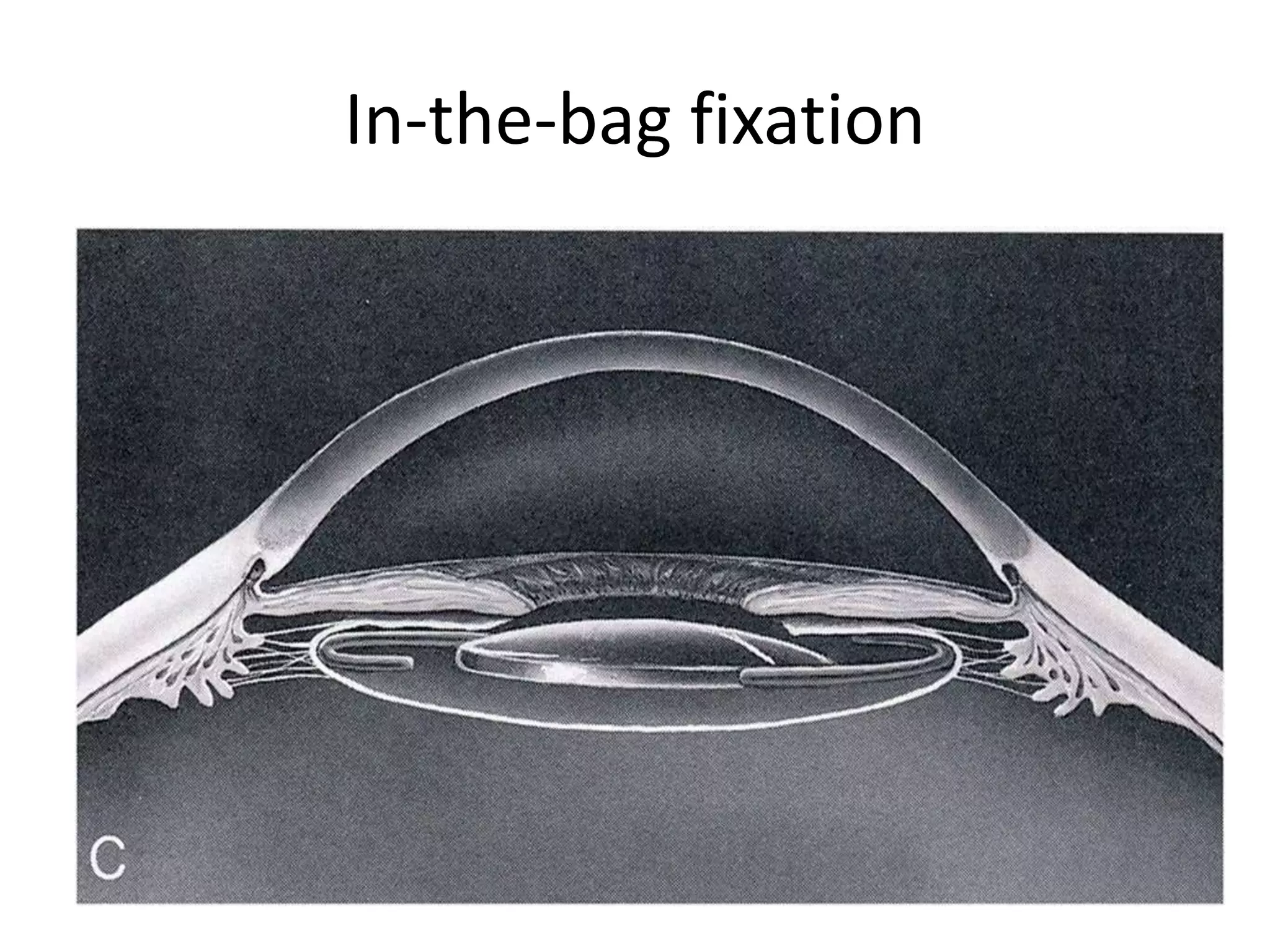


















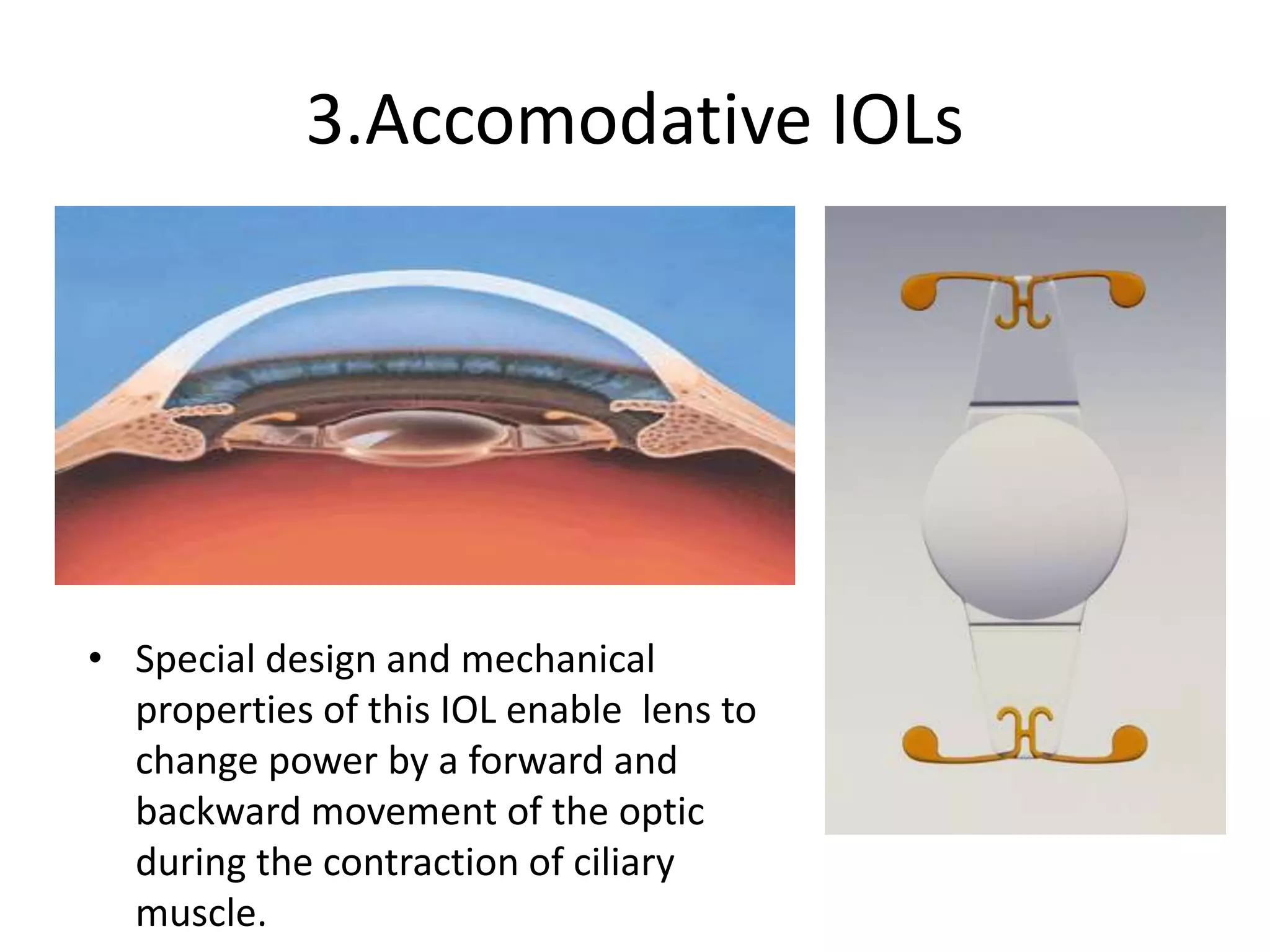

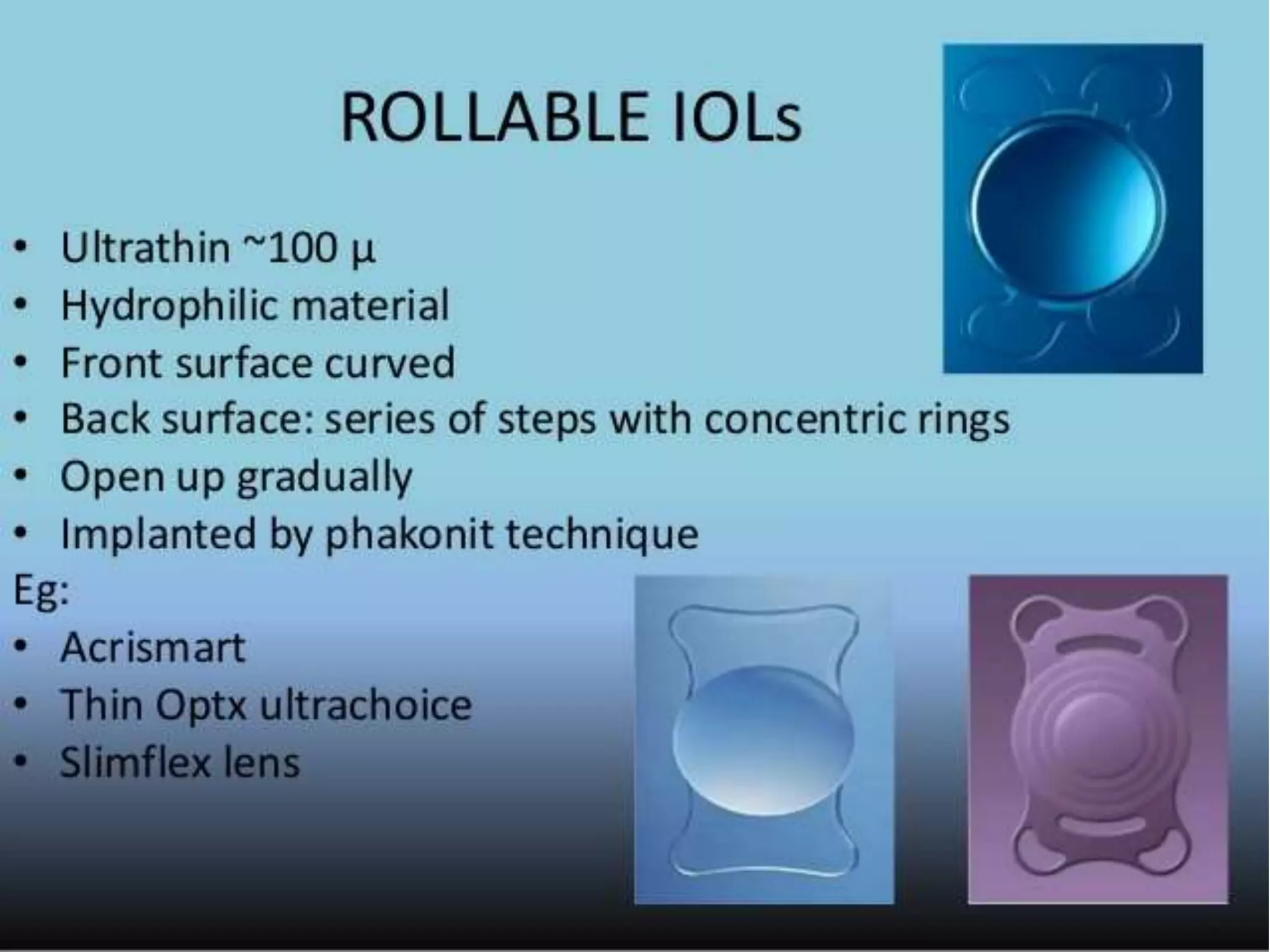







Types of intraocular lenses include foldable acrylic and silicone lenses. IOLs are either single piece or multipiece, and have different optic designs like aspheric, toric, or multifocal to correct vision. IOLs are implanted either in the capsular bag or ciliary sulcus, and are made of materials like acrylic, silicone, or hydrogels. Newer accommodating IOL designs aim to restore accommodation.





















































































