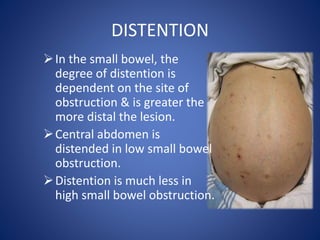
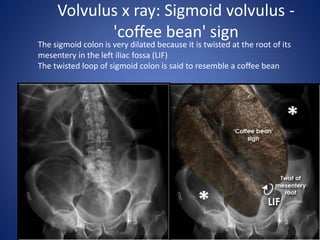
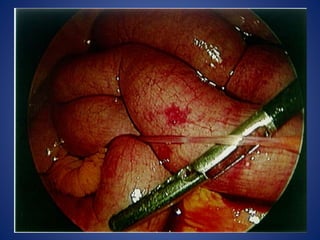
Intestinal obstruction occurs when intestinal contents cannot pass through normally. It can involve the small intestine, large intestine, or both. Obstruction is classified as mechanical, due to a physical blockage, or dynamic/adynamic without a blockage. Mechanical obstruction has specific causes and can be further classified as simple, strangulated, or closed loop based on vascular involvement. Clinical features vary depending on location and cause but commonly include pain, vomiting, distention, and constipation. Examination may reveal visible peristalsis, hyperactive bowel sounds, and tenderness.
![CLASSIFICATION
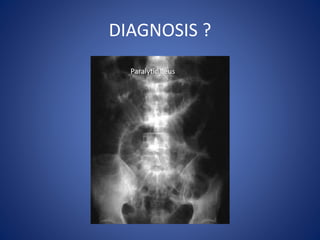
Dynamic/ Adynamic
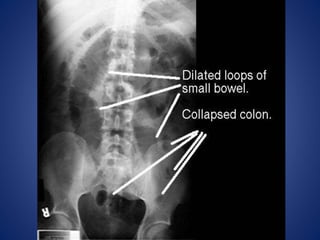
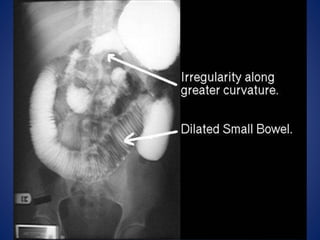
Small bowel obstruction [ high or low ]
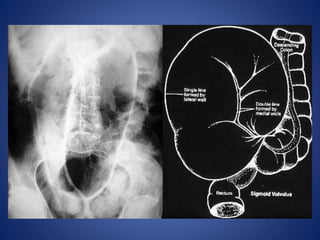
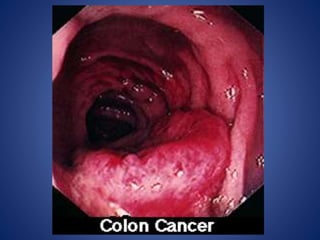
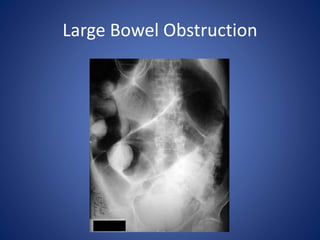
Large bowel obstruction
Acute
Chronic
Acute on chronic
Subacute
Simple
Strangulated
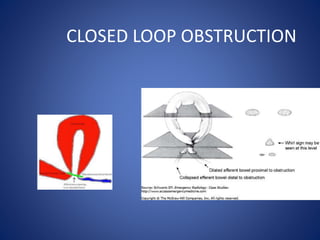
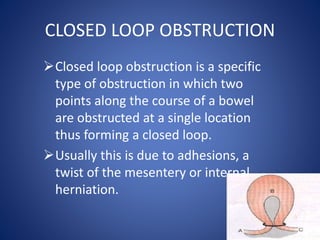
Closed loop obstruction](https://image.slidesharecdn.com/intestinalobstruction-170323180308-220826172708-87ccebf6/85/intestinalobstruction-170323180308-pdf-4-320.jpg)