CASE 1
•An elderlynursing home patient is brought to the
hospital with recent onset of colicky abdominal pain,
distension and constipation. On examination, the
abdomen is markedly distended and tympanic. There
is no marked tenderness. Plain abdominal x-ray shows
a markedly distended loop located mainly in the right
upper quadrant. Discuss the managements and
complications the patient can suffer
3.
CASE 2
• A45 YOF presents to the EMD for abdominal pain, nausea
and nonbloody vomiting for the past day. She has not had
any flatus during this time. She also endorses decreased
appetite. She has a past surgical history of cesarean section.
On P/E, there is diffuse tenderness to palpation of her
abdomen but no rebound tenderness or guarding. A supine
abdominal X ray shows dilated loops of small bowel. There
are no masses identified. Discuss the managements and
complications the patient can suffer.
CASE 1
• Anelderly nursing home patient is brought to the hospital with recent
onset of colicky abdominal pain, distension and constipation. On
examination, the abdomen is markedly distended and tympanic.
There is no marked tenderness. Plain abdominal x-ray shows a
markedly distended loop located mainly in the right upper quadrant.
Discuss the managements and complications the patient can suffer
6.
CASE 2
• A45 YOF presents to the EMD for abdominal pain, nausea and
nonbloody vomiting for the past day. She has not had any flatus
during this time. She also endorses decreased appetite. She has a past
surgical history of cesarean section. On P/E, there is diffuse
tenderness to palpation of her abdomen but no rebound tenderness
or guarding. A supine abdominal X ray shows dilated loops of small
bowel. There are no masses identified. Discuss the managements and
complications the patient can suffer.
7.
Learning Tasks
• DefineIO
• Risk factors/etilogy of IO
• Features and complications of IO
• Perform clinical assessment for a patient with Internal Obstruction
• Provisional and differential diagnosis
• Determine appropriate investigations to be perfomed to patients with
IO
• Treat, conduct follow up and refer the patients wit IO
• To provide preventive measures to patients with IO
Definition
Intestinal obstruction
• Failureof intestinal contents to pass through the bowel lumen
• Blockage of the passage of intestinal contents through the lumen of the
bowel
• When the intestinal contents fail t move distally, its called Intestinal
Obstruction.
• It’s the most common surgical emergency of the intestine
10.
Few important factsabout intestinal obstruction
• 80% occur in small bowel
• 20% occur in large bowel
• Majority (more than 80%) of small bowel obstructions are benign in
nature.
• In the large bowel, more than 70% of colonic obstruction is due to
malignancy-others being inflammatory bowel diseases, ileocaecal
tuberculosis, volvulus, etc.
11.
Causes
• Mechanical intestinalobstruction
• Also called dynamic obstruction
• Peristalsis is working against a mechanical obstruction
11
12.
Causes cont..
• Functionalintestinal obstruction
• Also known as adynamic obstruction
• May occur in two forms:-
• Paralytic ileus
• Absence of peristalsis
• Pseudo-obstruction
• Peristalsis is present in a non-propulsive form
12
13.
Mechanical / Dynamicobstruction
• Intraluminal causes
• In the lumen
• Intramural / Intrinsic causes
• In the wall of the gut
• Extramural / Extrinsic causes
• Outside the wall
13
14.
Intraluminal causes
• Faecolith
•Worms eg ascaris
• Gall stone
• Foreign body
• Polypoidal tumors
• Bezoars(partially digested materials)
14
Partial bowel obstruction
•Meaning that the lumen is narrowed but permits distal
passage of some fluid and air
• E.g. Richter's hernia in which a strangulated hernia
involving only one sidewall of the bowel, which can
result in bowel perforation through ischemia without
causing bowel obstruction
20
21.
Complete bowel obstruction
•In which there is complete mechanical blockage of the
normal progression of the intestinal contents
• In this case the intestinal lumen is totally occluded
• E.g. sigmoid volvulus
21
22.
Pathophysiology
• As aresult of obstruction, the proximal bowel undergoes
hyperperistalsis which is responsible for colicky pain abdomen.
• The peristalsis may continue for a few days and later the intestine
may be paralysed and flaccid. After 3-4 hours, distal to the
obstruction, all physiological activities of the bowel are stopped.
Intestine becomes contracted, pale and does not exhibit peristalsis.
• After a few hours, the proximal bowel gets dilated secondary to
obstruction.
23.
The causes ofdistension of intestinal loop are:
• A. Gaseous distension
• Swallowed air(70%).
• Because of colic and anxiety,the swallowed air is increased. Oxygen is
absorbed and nitrogen remains as it cannot be absorbed.
• This results in distension.
• Diffusion of air from the blood into bowel lumen increases carbon
dioxide which diffuses very rapidly.
• Gas due to bacterial activity releases H2S, NH3, et
24.
• B. Distensiondue to fluids
• 1500 ml of saliva
• 2 litres of gastric juice
• 3 litres of intestinal secretions
• l litre of bile and pancreatic juice
• Normally, all this fluid is absorbed in the bowel. In cases of intestinal
obstruction, this fluid absorption is delayed. It accumulates in the
intestinal loop. Excretion of water and electrolytes into the lumen is
also increased.
25.
• C. Roleof nitric oxide
• Activated neutrophils and macrophages accumulate within the
muscular layer of the bowel wall due to dilatation and inflammation
of the bowel wall.
• This damages the secretory and motor processes by release of
reactive proteolytic enzymes and cytokines.
• Net result is increase in the local release of nitric oxide, itself a potent
inhibitor of smooth muscle tone. It further aggravates the intestinal
dilatation.
26.
• D. Roleof bacteria
• Bacterial colony count increases following obstruction resulting in
stasis. From less than 106 in jejunum and from I08 in ileum, counts
increase.
• Bacterial translocation can occur even in simple obstruction without
strangulation. Thus, bacteria can enter into lymph nodes and into
systemic circulation
27.
• Abdominal distension,hypovolaemia, renal failure and sepsis set in.
• In addition to these changes, diaphragm gets elevated, respiration is
impaired which result in respiratory complications such as atelectasis
and basal pneumonia
• • In doubtful cases of viability, if facilities are available, a test called
fluorescein test can be done.
• 1000 mg of fluorescein is injected into peripheral vein and bowel is
inspected under Wood light. If loops are nonviable, resection and
anastomosis is done
28.
Strangulation
• Interference withblood supply: As the tension within the loops
becomes more and more, venous congestion takes place resulting in
oedema of the bowel wall.
• If the obstruction is not relieved, capillary rupture and haemorrhage
into bowel may ensue.
• In cases of volvulus and intussusceptions, the arterial supply gets
compromised rapidly causing gangrene of bowel wall very early.
• Bacterial proliferation takes place and endotoxins are released.
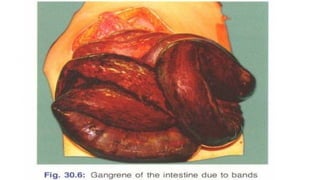
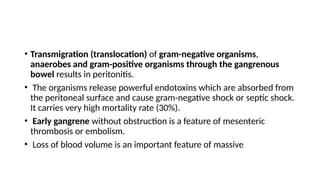
30.
• Transmigration (translocation)of gram-negative organisms,
anaerobes and gram-positive organisms through the gangrenous
bowel results in peritonitis.
• The organisms release powerful endotoxins which are absorbed from
the peritoneal surface and cause gram-negative shock or septic shock.
It carries very high mortality rate (30%).
• Early gangrene without obstruction is a feature of mesenteric
thrombosis or embolism.
• Loss of blood volume is an important feature of massive
Clinical features
• 1.Pain abdomen: Central abdominal pain is a feature of small intestinal
obstruction and peripheral pain is a feature of large intestinal obstruction.
• The pain is colicky in nature, lasts for 5-10 minutes and is intermittent. On
pressure, it decreases.
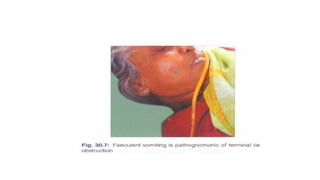
• 2. Vomiting is due to reverse peristalsis. Vomitus consists of stomach contents
initially, then bile, followed by faeculent matter. Faeculent is not faecal matter
but terminal ileal contents which undergo bacterial degradation and
fermentation resulting in the smell of faecal matter.
• Vomiting of altered blood indicates haemorrhage and gangrene. Frequent
vomiting reflects jejuna! obstruction
• Note: Vomiting of faeculent contents indicates terminal ilea/ obstruction.
35.
• 3:Distension ofthe abdomen: It may be central abdominal distension
as seen in ilea obstruction, peripheral abdominal as in large bowel
obstruction, or localised to one or two quadrants as in sigmoid
volvulus.
• 4. Constipation occurs because the distal bowel does not move.
Constipation to faeces and flatus is called obstipation.
• Absolute constipation is a cardinal feature of complete obstruction
where relative constipation is a feature of incomplete obstruction
36.
• Signs
1. Generalsigns of dehydration such as dryskin,drytongue, sunken eyes, feeble pulse, low
urinary output are seen. Dehydration occurs due to persistent vomiting and sequestration
of fluid and electrolytes. Hypokalaemia is an important finding.
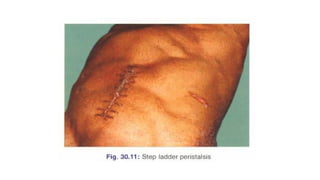
2. Abdominal findings
• Distension,tympanitic note on percussion
• Stepladder peristalsis is seen in terminal ileal obstruction. Right to left colonic peristalsis is
seen in left-sided
colonic obstruction, large bowel obstruction.
• On auscultation-loud, noisy intestinal sounds are heard. They are called borborygmi.
• Hernial orifices have to be examined, especially for Hernial orifices have to be examined,
especially for a femoral hernia in females.
37.
• WHAT ARETHE FINDINGS MAY APPEAR ON PER ABDOMINAL
EXAMINATION TO A PATIENT WITH INTESTINAL OBSTRUCTION
38.
38
Abdominal examination
• Abdominaldistension
• Visible peristalsis
• An old laparotomy scar
• Tender mass at one of his hernial orifice
• Abdominal tenderness
• A palpable abdominal mass
• Hyper-resonance
• Hyperactive bowel sounds occur early as GI contents attempt to overcome the
obstruction.
• Hypoactive bowel sounds occur late.
• Rectal examination
39.
Signs of strangulation
•It should be suspected when features of obstruction are
present along with features of shock.
• Features of septic shock-fever, hypothemia, renal failure,
• respiratory failure
• Rebound tenderness: It is called Blomberg's sign. It is a
classical sign of peritonitis.
• Guarding and rigidity of the abdominal wall.
• Absent bowel sounds because rest of the bowel loops
undergo paralytic ileus.
• Sudden symptoms-spasmodic pain (due to peristalsis) and
continuous pain suggest strangulation
• Features of strangulation and perforation occur quickly in
cases of closed loop obstruction
43.
Rectal examination
• Insmall bowel obstruction, rectum is empty and is often ballooned
out
• Carcinomatous growth with or without stools can be felt.
• •The finger may be stained with blood.
• The small intestine is considered dilated if loops of bowel measure
more than 3 cm in diameter.
• Measurements for the large bowel vary among different anatomic
segments, with a relative threshold of 9 cm in diameter for the
proximal colon and 5 cm for the sigmoid colon.
INVESTIGATIONS
• Complete bloodpicture: Low Hb% indicates underlying malignancy. Increased
total WBC count indicates infection and sepsis (perforation).
• Electrolytes: Most of the electrolytes are low in cases of intestinal obstruction
and require con-ection preoperatively. Strangulation may be associated with
deranged potassium,
• LFT- amylase or lactic dehydrogenase.
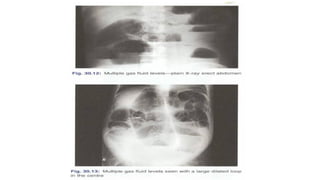
• Plain X-ray abdomen in the erect position may show
multiple gas fluid levels. Gas levels appear earlier than fluid level. Normally,
two insignificant fluid levels can be present, one in the terminal ileum and one in
the first part of the duodenum.
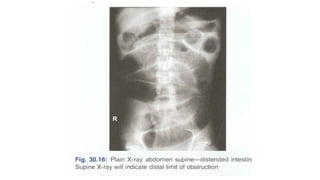
• Supine films indicate the distal limit of obstruction .
49.
MANAGEMENT
• Preoperative preparationincludes correction of dehydration,
electrolytes and broad spectrum antibiotics.
• Principles in the management of intestinal obstruction are as
follows:
• A. Aspiration with Ryle's tube. This is the most important step in the
management of intestinal obstruction.
• It helps in decreasing the distension and also prevents vomiting. This
will help in preventing respiratory complications, such as aspiration
following general anesthesia
50.
• B. Bowelcare: No purgatives because purgation can cause perforation.
• C. Charts: Temperature, pulse, respiration and intake-output chart. In
cases of conservative management such as obstruction due to adhesions,
change in temperature and increasing pulse rate suggests perforation or
gangrene. These cases have to be explored immediately.
• D. Drugs to cover gram-positive, gram-negative and anaerobic
organisms.
• E. Exploratory laparotomy is done and depending upon the findings,
obstruction is treated. A few examples are given in
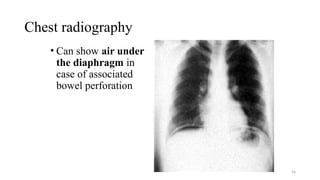
Chest radiography
• Canshow air under
the diaphragm in
case of associated
bowel perforation
56
57.
Abdominal radiographs
• 2views are required which are Supine and Erect
• Dilated bowel loops with air-fluid levels indicate Intestinal
obstruction
• Able to show the level of obstruction
• Small bowel lie centrally and colon peripherally
58.
Abdominal radiographs cont..
•Jejunal obstruction shows valvulae conniventes i.e. parallel lines
spanning the entire width of the bowel lumen
• Obstructed ileum appears cylindrical with less clearly valvulae
conniventes
• Obstructed colon shows dilated bowel with haustral markings
60
Contrast studies
• Thisis valuable in detecting presence of obstruction and in differentiating
partial from complete blockages.
• This study is useful when plain radiographic findings are normal in the
presence of clinical signs of IO or if plain radiographic findings are
nonspecific.
• 2 types of Contrast agents used in this study-water insoluble CM eg
barium or water soluble CM eg Gastrografin
• Barium is commonly used -It is safe and useful when diagnosing
obstructions provided no evidence of bowel ischemia or perforation exists
Conservative treatment
• Includes:-
–Correctionof fluid and electrolyte
imbalance(initially; crystalloids RL,NS)
–Nasogastric Tube (for decompression,
decrease vomiting, prevent APNA)
–Nil per oral( Relief of obstruction)
–Prophylactic antibiotics
–Analgesics
• Urethral catheterization for recording urine
output
64
65.
Conservative treatment cont..
•Other modalities include:-
• Decompression of sigmoid volvulus with a sigmoidoscope
• Hydrostatic reduction of intussusception with a contrast
enema
• Endoscopic or radiological placement of metal stent
66.
Surgical treatment
Indications forsurgical interventions
• Failure of conservative treatment
• Presence of underlying disease process that must be treated e.g. hernia,
obstructing tumor
• Signs of peritoneal irritations
NOTE; Conservative treatment should not continue beyond 72 hours, if no relief SURGICAL
INTERVENTION
66
67.
Preoperative care
• IVfluid resuscitation with crystalloid fluids
• NGT
• Nil orally
• Prophylaxis antibiotics
• Analgesics
• Pre-anesthetic visit
• Informed written consent
67
68.
Preoperative care cont…..
•Monitor
–Urine output [normal=
–Input-output
–Vital signs [T, PR, RR, BP]
–The volume of NGT
68
Case 3
• A65YOM presents to the hospital for increased abdominal pain and
distension. He has a history of diverticulosis and chronic constipation.
He last had a bowel movement 1 week ago and has not had any
flatus in the past day. He reports 2 episodes of vomiting at home. On
p/e his abdomen is distended and there is diffuse tenderness on
palpation. Erect abdominal x ray revealed air under the diaphragm
and dilated loops with a suspicious mass at the transition point. What
are the managements regarding this information.
72.
Key points
• Intestinalobstruction is defined as a blockage of the
passage of intestinal contents through the lumen of the
bowel
• The cause of intestinal obstruction can be grouped into
dynamic causes and adynamic causes.
• Treatment of intestinal obstruction can be either
conservatively or requiring surgical intervention.
73.
Review questions
1. Whatis intestinal obstruction?
2. What are the causes of intestinal obstruction?
3.What are the clinical features of intestinal
obstruction?
4. Outline management of intestinal obstruction?
73
74.
References
• S.DAS,A Manualon clinical surgery 2011
• Bailey &Love’s short Practice of Surgery 26th
Edition
• SRB_s Manual of Surgery
• Surgery Notes from Prof. Aziz, compiled by Dr. Ndile 2003.MNH,Pg
61-66.




![Functional intestinal obst. [cont’d]
• Infectious
• Peritonitis
• Vascular
• Mesenteric ischaemia
• Pharmacological
• Anticholinergics (atropine)
• Opiates (morphine, codein)
• Antipsychotics (amytriptine)
18](https://image.slidesharecdn.com/2-250421211851-e8b2ef51/85/2-INTESTINAL-OBSTRUCTION-Surgical-pptx-18-320.jpg)





![Preoperative care cont…..
• Monitor
–Urine output [normal=
–Input-output
–Vital signs [T, PR, RR, BP]
–The volume of NGT
68](https://image.slidesharecdn.com/2-250421211851-e8b2ef51/85/2-INTESTINAL-OBSTRUCTION-Surgical-pptx-68-320.jpg)








































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)






