DEFINITION: is wheneither the small or large
intestine luminal content is patholologically partly
or completely blocked, thus prevents food, fluids,
and gas from moving through the intestines distally
in the normal way.
CLASSIFICATION: There is two types of intestinal
obstruction:
1)- Mechanical: peristalsis is working against a
mechanical obstruction.
2)- Functional: Peristalsis is absent (paralytic or
adynamic ileus) a mechanical element is absent.
3.
MECHANICAL OBSTRUCTION:Can be classified according to:
1)- Evolution:
a)-Acute: usually occurs in small bowel over hours to
days and has a rapidly evolving course.
b)-Chronic: is usually seen in large bowel with a slow
course, lower abdominal colic and constipation, followed by
distension and malnutrition.
2)-Clinically: a)- Small bowel obstruction:
i)- High: ( above Treitz ligament ), vomiting
occurs early and is profuse with rapid dehydration. Distension is
minimal with little evidence of fluid levels on abdominal radiography.
ii)- low: ( from Treitz ligament to ileocecal
junction ), pain is predominant with central distension. Vomiting is
delayed, and multiple central fluid levels are seen on radiography.
b)- Large bowel obstruction: distension is early and
pronounced. Pain is mild and vomiting and dehydration are late.
4.
3)- Physiologic impact:
a)-Simple obstruction: where the
blood supply is intact.
b)- Strangulating obstruction: there is
direct interference to blood supply (hernial rings,
intra-peritoneal adhesions/bands, volvulus).
c)- Close loop obstruction: Both limbs
of the bowel are obstructed, therefore, gas and
fluids can not pass in either direction.
e)- Perforating obstruction: The bowel
proximal to the obstruction overdistends and
perforates.
5.
Functional obstructions:
•There is impaired motility.
• Causes include:
Generalized peritonitis.
Postoperative ileus(3 to 7 days after surgery).
Retroperitoneal hematoma.
Nerve root compression.
Nephrectomy.
Electrolytes disbalances( hypokalemia).
Pneumonia.
Critical patients ( severe burns, multiple
trauma,etc).
Urine tract infections.
• Usually treated by observation, intravenous fluids and electrolytes
imbalances correction, nasogastric suction, and nutritional support.
6.
Etiology:
1)-Intraluminal:
Impacted feces.
Foreignbodies.
Bezoars.
Gallstones.
Parasites.
2)-Intramural: Benign tumors i.e.
lipoma(intussuspception).
Malignancies. ( 3rd
).
Inflammatory strictures( Crohn`disease, ulcerative colitis, TB,
radiation injury.
3)-Extramural:
Intraperitoneal bands and adhesions. ( 1st
).
Hernias (external or internal). ( 2nd
).
Volvulus.
Intussusception.
Large intraabdominal tumors or abscesses.
7.
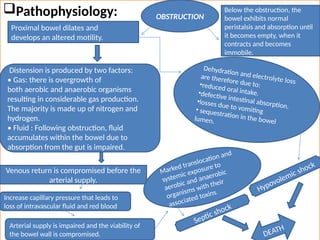
Pathophysiology:
Proximal bowel dilatesand
develops an altered motility.
OBSTRUCTION
Below the obstruction, the
bowel exhibits normal
peristalsis and absorption until
it becomes empty, when it
contracts and becomes
immobile.
Distension is produced by two factors:
• Gas: there is overgrowth of
both aerobic and anaerobic organisms
resulting in considerable gas production.
The majority is made up of nitrogen and
hydrogen.
• Fluid : Following obstruction, fluid
accumulates within the bowel due to
absorption from the gut is impaired.
Dehydration and electrolyte loss
are therefore due to:
•reduced oral intake.
•defective intestinal absorption.
•losses due to vomiting
• sequestration in the bowel
lumen.
Venous return is compromised before the
arterial supply.
Increase capillary pressure that leads to
loss of intravascular fluid and red blood
Arterial supply is impaired and the viability of
the bowel wall is compromised.
Marked translocation and
systemic exposure to
aerobic and anaerobic
organisms with their
associated toxins.
Septic shock
Hypovolemic shock
DEATH
8.
Clinical features:
• Thereare four cardinal features:
Pain.
Vomiting.
Distension.
Constipation.
• These features vary according to:
The location of the obstruction.
The age of the obstruction.
The underlying pathology.
The presence or absence of intestinal ischemia.
9.
• Other manifestationsinclude:
Dehydration.
Oliguria.
Hypovolemic shock.
Pyrexia.
Septicemia.
Respiratory embarrassment.
Peritonism.
• In all cases of suspected intestinal obstruction, all
hernial orifices must be examined.
10.
Pain:
• Is thefirst symptom.
• May occurs suddenly.
• Usually is severe.
• It is colicky in nature.
• The pain coincides with increased peristaltic
activity.
• The colicky pain is replace by a mild, constant,
diffuse pain.
• The development of severe and continuos pain
indicates strangulation or peritonitis.
• Does not occur in paralytic ileus.
11.
Vomiting:
• The moredistal the obstruction, the longer the
interval between the onset of nausea and vomiting.
• In proximal obstruction may be profuse and
unassociated with abdominal distention.
• As obstruction progresses the character of the
vomits changes from digested food to feculent
material due to the presence of enteric bacterial
overgrowth.
• In distal obstruction is less frequent and feculent
the large bacterial population of intestinal contents.
12.
Distension:
• In thesmall bowel the degree of distension is
dependent on the site of the obstruction.
• Is greater the more distal the lesion.
• Visible peristalsis may be present ( Bouverest`sign ).
• Increased bowel sounds occur early as GI contents
attempt to overcome the obstruction.
• Hypoactive bowel sounds occur late.
• It is delayed in colonic obstruction.
• Minimal or absent in the presence of mesenteric
vascular occlusion.
• Markedly evident and asymmetric in sigmoid volvulus.
13.
Constipation: This maybe classified as:
• Absolute, when neither faeces ner flatus is passed
( Obstipation ).
• Relative (where flatus only is passed).
• Absolute constipation is a cardinal feature of complete intestinal
obstruction.
• Some patients may pass flatus or faeces after the onset of
obstruction due to the evacuation of distal bowel contents.
• The rule that constipation is present in intestinal obstruction
does not apply in:
Richter’s hernia.
Gallstone obstruction.
Mesenteric vascular occlusion.
Obstruction associated with a pelvic abscess.
Partial obstruction (fecal impaction/colonic
neoplasm) where diarrhoea may be present.
14.
Other manifestations:
Dehydration:
• Isseen most commonly in small bowel obstruction
due to vomiting and fluid sequestration.
• Results in dry skin and tongue.
• Poor venous filling.
• Sunken eyes.
• Oliguria.
Hypokalaemia:
• Is not a common feature in mechanical obstruction.
• Often seen in paralytic ileus.
15.
Pyrexia: in thepresence of obstruction may
indicate:
• The onset of ischemia.
• Intestinal perforation.
• Inflammation associated with the obstructing
disease.
Hypothermia: indicates septic shock.
Abdominal tenderness: indicates:
Ischemia.
Peritonitis.
Perforation.
16.
Investigations:
• Radiographs areessential to confirm the diagnosis
and accurate the site of the obstruction.
• The radiological diagnosis is based on a
supine(erect) abdominal radiograph.
• If conditions of the patient are poor a lateral
decubitus position view may be taken.
• Usually can determine whether small bowel, colon
or both are distended.
• Radiographs show multiple gas-fluids levels, with
distended bowell resembling an inverted U.
19.
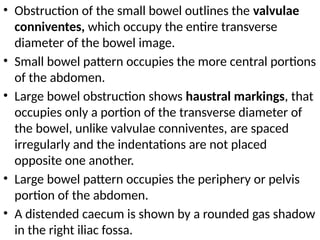
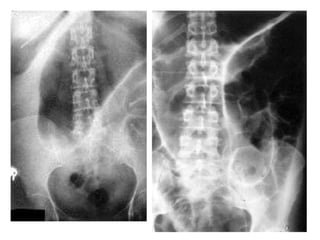
• Obstruction ofthe small bowel outlines the valvulae
conniventes, which occupy the entire transverse
diameter of the bowel image.
• Small bowel pattern occupies the more central portions
of the abdomen.
• Large bowel obstruction shows haustral markings, that
occupies only a portion of the transverse diameter of
the bowel, unlike valvulae conniventes, are spaced
irregularly and the indentations are not placed
opposite one another.
• Large bowel pattern occupies the periphery or pelvis
portion of the abdomen.
• A distended caecum is shown by a rounded gas shadow
in the right iliac fossa.
22.
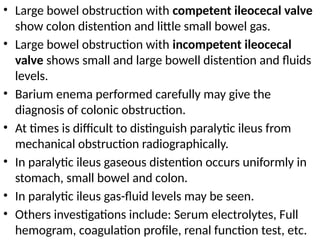
• Large bowelobstruction with competent ileocecal valve
show colon distention and little small bowel gas.
• Large bowel obstruction with incompetent ileocecal
valve shows small and large bowell distention and fluids
levels.
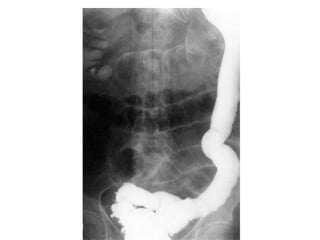
• Barium enema performed carefully may give the
diagnosis of colonic obstruction.
• At times is difficult to distinguish paralytic ileus from
mechanical obstruction radiographically.
• In paralytic ileus gaseous distention occurs uniformly in
stomach, small bowel and colon.
• In paralytic ileus gas-fluid levels may be seen.
• Others investigations include: Serum electrolytes, Full
hemogram, coagulation profile, renal function test, etc.
24.
Treatment:
• Supportive treatment:
1)-Gastrointestinal drainage.
2)- Fluid and electrolytic replacement.
3)- Antibiotics.
4)- Oxigentherapy.
• Surgical treatment:
Necessary for most of the cases.
Should be done when resuscitation is complete,
provided there is no:
sign of strangulation.
closed-loop obstruction.
25.
1)- Gastrointestinal decompression:
•Is achieved by the passage of a nasogastric
tube(Levine) or long intestinal tube(Miller-Abbott).
• The tubes are normally placed on free drainage,
with 4-hourly aspiration.
• Also reduce the risk of aspiration.
2)- Fluid and electrolytic replacement:
• The basic biochemical abnormality is sodium and
water loss, therefore the appropriate replacement
is Hartmann’s solution or normal saline.
• Administration of blood, plasma, or both should be
considered if strangulation is suspected.
26.
3)- Antibiotics:
• Broad-spectrumantibiotics are given because of
bacterial overgrowth.
• Antibiotic therapy is mandatory for all patients
undergoing small or large bowel resection.
4)- Oxigentherapy:
• The goal is reduce exchange with nitrogen within
bowel lumen.
27.
Surgical treatment:
• Thetiming of operation depends upon three
factors:
a)-Duration of obstruction(severity of fluid,
electrolyte, and acid-base disturbances).
b)- Improvement of vital organs function(cardiac,
renal failure. Shock,etc.).
c)- Risk of strangulation and perforation.
• Indications of early operation:
a)- Obstructed or strangulated external hernia.
b)- Internal intestinal strangulation.
c)- Acute obstruction.
28.
• If thesite of obstruction is unknown, adequate
exposure is best achieved by a midline incision.
• Operative assessment is directed to:
the site of obstruction.
the nature of the obstruction.
the viability of the gut.
• Identification of the caecum is the best initial
maneuver:
If it is collapsed, the lesion is in the small bowel.
If dilated indicates large bowel obstruction.
29.
• The criteriaused in determining bowel viability are:
a)- Color
b)- Motility
c)- Arterial pulsation.
• Intestinal adhesions are treated by division or lysis of the
obstructcting bands(adhesionlysis).
• Hernias are treated by a reduction of the contents and
repair.
• Intestinal tumors are treated by resection and anastomosis.
• Intussusception: reduction is achieved by squeezing the
most distal part of the mass in a cephalic direction. Do not
pull.
• If irreducible or gangrenous intussusception the mass
should be excised and an anastomosis performed.
30.
• Gallstones, worms,trichobezoars and phytobezoar,
and others foreign bodies: when possible, may be
kneaded into the caecum, otherwise open removal is
required.
• Volvulus of the small bowel: is treated by reduction of
the twist if there is not ischemia.
• Caecal volvulus: the volvulus should be reduced, and
fixation of the caecum to the right iliac fossa
(caecopexy). If the caecum is ischemic or gangrenous a
right hemicolectomy is performed.
• Sigmoid volvulus: when the bowel is viable, fixation of
the sigmoid colon to the posterior abdominal wall.
Sigmoid colectomy and end to end anastomosis, or end
colostomy.
31.
• Malignancies ofthe caecum can be treated by ileo-
transverse by pass, or excision by right hemicolectomy and
ileo-transverse anastomosis.
• Left colon obstructions entails three steps:
1)- Proximal colostomy to the obstruction to relief gaseous distention.
2)- Resection of the affected segment and anastomosis, leaving
colostomy intact.
3)- Closure of colostomy when healing of anastomosis is complete.
• Also can be done resection and creation of either end
colostomy or double barreled colostomy and closure of the
colostomy in a second operation.
• Stents are expandable metal tubes in some cases of
obstruction may be placed in the large bowel to help
intestinal contents move forward as palliative method or to
improve conditions of the patient previous to surgery.
32.
Intestinal obstructionof the newborn:
• Neonatal intestinal obstruction has an approximate
incidence of 1:2000 live births.
• Congenital atresia and stenosis are the commonest causes.
• Volvulus neonatorum, meconium ileus and Hirschsprung's
disease may also be responsible.
Congenital atresia:
• Incidence according with anatomical site:
•duodenum--35 per cent.
•jejunum--15 per cent.
•ileum--25 per cent.
•ascending colon--10 per cent.
• multiple sites--15 per cent.
• Surgery is required as soon as resuscitation is complete.
33.
Meconium ileus:
• Isthe neonatal manifestation of cystic fibrosis.
• Abdomen radiograph reveal a distended small
intestine with mottling.
• Fluid levels are generally not seen.
• Assessment includes:
Absence of trypsin from stool or bile.
Concentration of sodium chloride in sweat greater
than 80 mmol/litre.
Negative immunoreactive blood trypsin estimation.
• If conservative management fails, laporotomy is
indicated.
34.
Hirschsprung’s disease:
• Thisis due to failure of complete migration of the
ganglion cells of the large bowel to the anus.
• This results in an aganglionic segment producing
physiological obstruction.
• 80 per cent present in the neonatal period with acute
large bowel obstruction.
• 20 per cent present with failure to thrive or severe
constipation.
• Barium enema reveals a characteristic narrow segment.
• A full-thickness rectal biopsy will show absence of
ganglion cells.
• Treatment consists of an initial loop colostomy followed
by a definitive pull-through procedure.



















































![carotid stenosis [Autosaved].pptx for master students](https://cdn.slidesharecdn.com/ss_thumbnails/carotidstenosisautosaved-241229032708-f20dd02c-thumbnail.jpg?width=640&height=640&fit=bounds)



















