INTRODUCTION
Intestinal obstructionoccurs when the normal propulsion and
passage of intestinal contents does not occur.
Intestinal obstruction is failure of forward flow or distal propagation
of intestinal contents.
These intestinal contents include the 4 “F’s”- Food, Fluid, Faeces,
Flatus.
It is also known as bowel obstruction or ileus
In broadest terms, it includes both mechanical obstruction and
intestinal paralysis (aka paralytic ileus)
Any portion of the gastrointestinal tract can be involved.
4.
• It doesnot typically include gastric outlet obstruction or
oesophageal obstruction.
• ●Intestinal obstruction is considered a surgical emergency
depending on the cause or aetiology
• ●It is one of the common causes of acute abdomen in our
environment.
5.
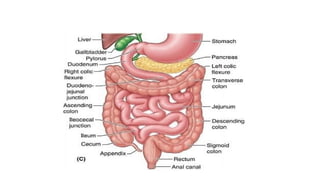
RELEVANT ANATOMY
• Thesmall intestine lies between the stomach and the large intestine
and comprises the duodenum, jejunum and ileum.
• Presence of mesentery except in the duodenum
• Branches of the abdominal aorta- celiac trunk, superior mesenteric
artery and inferior mesenteric artery.
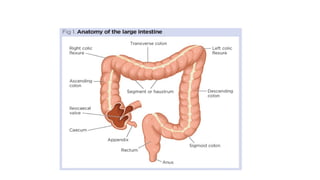
• Large intestine- cecum, appendix, ascending, transverse, descending,
and sigmoid colon, rectum and anal canal.
8.
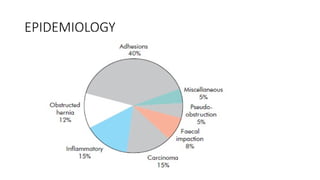
EPIDEMIOLOGY
• It isone of the commonest causes of acute abdomen worldwide.
• No racial predilection
• M > F
• Incidence increases with age
CLASSIFICATION
• It canbe classified based on
1. Mechanism of obstruction
2. Site of obstruction
3. Nature of obstruction
4. Degree of obstruction
5. cause of obstruction
11.
• 1. BASEDON MECHANISM OF OBSTRUCTION
• Mechanical intestinal obstruction(aka dynamic
obstruction)- There is an initial normal
or exagerrated peristaltic wave which attempts to
overcome a physical occlusion of the intestinal tract.
• Paralytic Ileus (aka adynamic obstruction)- there
is atony and loss of peristalsis from compromised
gut innervation in the absence of physical bowel occlusion.
12.
BASED ON ONSET(Further classification of mechanical)
• Acute:- sudden onset of manifestation measured in minutes to hours
(e.g. volvulus-Sigmoid, small bowel, caecal, ileo-sigmoid knotty)
• Chronic:- gradual onset of manifestation measured in days to weeks.
Occurs especially in the elderly in the setting of left sided large bowel
obstruction
• Acute on chronic:- e.g. large bowel neoplasm with super imposed
fecal impaction or oedema
13.
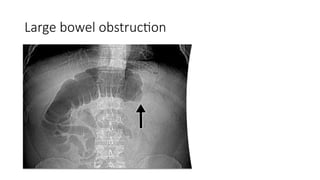
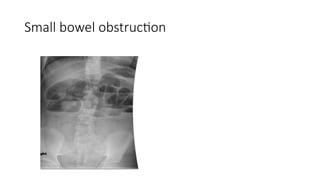
2. BASED ONSITE OF OBSTRUCTION
• It can be small bowel vs large bowel (important in nature of surgical
intervention).
Common Small bowel lesions include hernias, volvulus, adhesions.
Common large bowel lesions include colorectal tumours, sigmoid volvulus,
faecal impaction
• It can also be proximal /high obstruction vs distal / low obstruction
(important in evaluating the nature and extent of fluid and electrolyte
derangements)
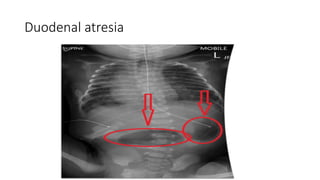
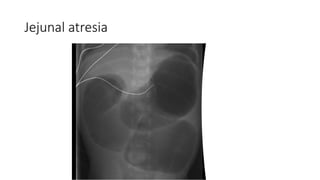
• High obstruction can occur at the level of proximal ileum, jejunum or
‘duodenum’
• Low obstruction involves the terminal ileum, colon or rectum.
14.
3. BASED ONNATURE OF OBSTRUCTION
• Simple obstruction:- single site of luminal occlusion without compromise of bowel
blood supply
• Closed loop obstruction :- at least 2 sites of luminal occlusion with an intervening
segment of bowel distention e.g. obstructed hernia, volvulus, obstruction of
ascending colon with a competent ileocecal valve which can cause cecal
perforation
• Strangulated obstruction :- in addition to the occlusion of the lumen, the blood
supply to the segment of bowel involved is also cut off. E.g. strangulated inguinal
hernia. luminal obstruction with associated compromise of bowel blood supply.
15.
4. BASED ONDEGREE OF OCCLUSION
Partial obstruction:- Passing flatus but not faeces, presence of gas
shadow in the pelvis on abdominal imaging(80% will can resolve non
operatively)
Complete obstruction:- No passage of flatus or faeces, absence of gas
in pelvis. (80% will require operative intervention)
17.
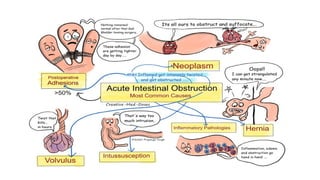
AETIOLOGY
The causes ofmechanical intestinal obstruction include the following:-
Intraluminal lesions- Foreign body, impacted feaces, pendunculated polyps,
gall stone ileus, ascaris, bezoars(tufts of hair)
Intramural lesions- tumors(carcinoma,leiomyoma,leiomyosarcoma),
inflammatory pathologies(ileocecal TB, IBD), intussusception,
volvulus(controversial: intramural vs extramural)
Extramural lesions- external hernias(commonest is inguinal),adhesions(post
op,post inflammatory or congenital),internal hernias, solid intrabdominal
masses
PATHOPHYSIOLOGY
● With theonset of intestinal obstruction depending on the site, 2
events happen distal to the obstruction; continuous propagation of
distal contents until it is excreted or absorption of the distal
contents
● Both events lead to the collapse of the distal segment of bowel, the
onset of which depends on the site of obstruction(e.g. jejunum vs
rectum)
● Proximal to the site of obstruction, accumulation of gas and fluid
occurs.
● The sources of the gas include swallowed air(main source), diffusion,
fermentation/putrefaction by intestinal bacteria.
20.
PATHOPHYSIOLOGY
• The sourceof fluid proximal to the obstruction is mainly from GI
secretions.
• Total possible fluid accumulation is 7-10 L per day.
• The combination of accumulated gas and fluid will cause increased
resting intraluminal pressure from 2-4 mmHg to 10mmHg in small
bowel and 25mmHg in large bowel
• The increased intraluminal pressure will compromise venous drainage
and the increased venous pressure will lead to extravasation of fluid
in 3 sites: bowel wall(oedema),lumen and peritoneum
21.
PATHOPHYSIOLOGY
• The extravasationof fluid in these 3 sites further increases
intraluminal pressure
• A major problem with bowel wall oedema is decreased absorption
& increased secretion of H2O, Na+
and K+
with associated fluid,
electrolyte and acid-base imbalance.
• This is in the form of hypovolemia(+/- shock=ARF),hyponatremia,
hypokalaemia, metabolic acidosis(low obstruction) or metabolic
alkalosis(high obstruction)
22.
PATHOPHYSIOLOGY
● Further increasein intraluminal pressure affects the capillaries
leading to petechieal haemorrhage on the gut mucosa and
microperforations
● Later the intraluminal pressure causes dilatation of lymphatics with
associated bacterial translocation and sepsis
● Arterial compromise occurs lymphatic obstruction and leads to
strangulation and gangrenous bowel.
● Gross abdominal distention leads to splinting of the diaphragm
potential respiratory acidosis and respiratory failure.
HISTORY
Cardinal symptoms
● Abdominalpain (colicky and central in mechanical obstruction; dull,
vague and diffuse in paralytic ileus)
● Vomiting(bilious vs feculent; high vs low obstruction)
● Abdominal distention(high vs low obstruction)
● Constipation/obstipation
A history of previous abdominal or pelvic surgery, cancer treatment,
chronic medical illness and medication is also important.
25.
• If highobstruction, patient may present more with vomiting early and
distension is minimal.
• In low obstruction, patient may present more with abdominal pain
and central distension. Vomiting is delayed.
• In large bowel obstruction, distension is early and pronounced. Pain is
moderate and vomiting is late.
TREATMENT
• Initial management/nonoperative intervention for all patients include the
following
1. Admit into the emergency room for resuscitation and evaluation
• Check Airway patency, Breathing and Circulation
2. NPO: To prevent worsening of increased intraluminal pressure
3. Nasogastric decompression: gastric aspiration must be done to remove swallowed
air and intestinal contents which regurgitate into the stomach. This reduces the
distension of the bowel thereby minimizing the intestinal secretion of water and
electrolytes. It helps to decrease distension, prevent aspiration and monitor effluent
4. IV fluid resuscitation — Normal saline or Ringers' lactate is given as anti-shock
(20mls/kg) if there is shock and then continued as maintenance fluid for the first 24
hours in adults.
34.
5. Urethral catheterto monitor urine output(note normal values)
6. IV Antibiotics: spread of bacteria should be prevented or checked
with broad spectrum antibiotics such as ciprofloxacin and
metronidazole or ceftriaxone.
7. Analgesia after resuscitation once definitive line of intervention
decided
8. Adequate monitoring of vital signs
9. Nurse in cardiac position especially if risk of diaphragmatic splinting
or aspiration pneumonitis.
35.
Surgical Intervention
• Indicationsfor surgery
1. Peritonitis
2. Strangulation
3. Persisting shock despite rehydration
4. Failed conservative management
5. Evidence of peforation
• Exploratory Laporotomy + Surgical treatment of cause
1. Adhesions: adhesiolysis and resect non viable bowel loops and do anastomosis
2. Bands – release/ligate the band
3. Tumour- resect, do end to end anastomosis if benign
36.
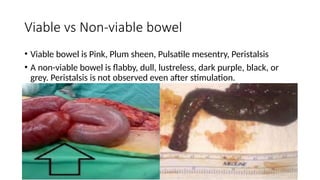
Viable vs Non-viablebowel
• Viable bowel is Pink, Plum sheen, Pulsatile mesentry, Peristalsis
• A non-viable bowel is flabby, dull, lustreless, dark purple, black, or
grey. Peristalsis is not observed even after stimulation.
CONCLUSION
• Intestinal obstructionis an emergency which should be attended to
without any delay.
• Prompt diagnosis and treatment will reduce significant morbidity and
mortality.
39.
REFERENCES
• Baja’s principlesand practice of surgery.
• Gautam D. (2006). Intestinal obstruction. Retrieved from SlideShare.
• Medscape.
• Clinical surgery tutorial manual