Vital signs:
• BP128/78 BT 36.8 PR 72 RR 20
General appearance:
• Good consciousness , awake , well-cooperated
• HEENT:
• Not pale conjunctivae , Anicteric sclerae
PHYSICAL EXAMINATION
9.
PHYSICAL EXAMINATION
Chest:
• clearand equal breath sound both lungs
Heart:
Pulse full and regular , normal S1,S2 , no murmur
Abdomen:
Soft , Not tender
10.
Musculoskeletal
Left Hip :Not tender , Limit ROM all direction due to pain
(especially when abduction)
Right Hip : Not tender , Full ROM
Back : Not tender , no stepping
Neurologic
GCS E4V5M6
Pupil 3 mm RTLBE, Full EOM
Motor power grade V all extremities
PHYSICAL EXAMINATION
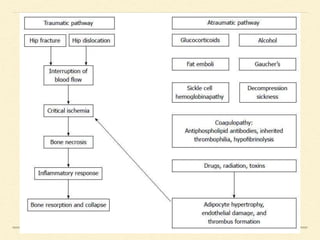
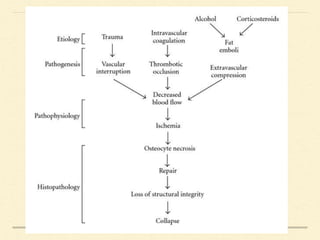
DEFINITION
The avascular stateof the necrotic bone that result from
loss of circulation from numerous potential cause
Also known as avascular necrosis , aseptic necrosis ,
atraumatic necrosis , ischemic necrosis
19.
EPIDEMIOLOGY
20,000 – 30,000new cases per year in the United States
accounts for 10% of total hip arthroplasties performed
Average age at presentation is 35 to 50
bilateral hips involved 80% of the time
SYMPTOMS
• Typically asymptomaticin early course
• Pain
• Groin pain (most common) , thigh pain , buttock
pain
• Weight bearing or motion-induced pain is found
in most cases
• Rest pain approximately 2/3 of patients, Night
pain 1/3
• Pain in multiple joint (Rare)
25.
PHYSICAL EXAM
Limited rangeof motion at the hip and
complain of pain particularly with forced
internal rotation and abduction
A limp may be present in the late course
PLAIN RADIOGRAPHY
May appearnormal in early stage
Increased radiolucency in the femoral head
Pathognomonic crescent sign (Subchondral radiolucency)
Femoral head collapse
Severe arthritic changes
MRI
Imaging of choicefor earlier stages of osteonecrosis of the
femoral head
Determination of the exact stage and extent of the
pathologic process without use of invasive method
Useful in following the progression of the asymptomatic
disease and in evaluating the efficacy of treatment
30.
BONE SCAN
Bone scanningcan occasionally be useful , when the
patient has a C/I to MRI or when assessing the status of
multiple other joint
The uptake of technetium-99m usually decreased in very
early stage and is variable or increased at a stage when
symptoms occur
31.
CLASSIFICATION
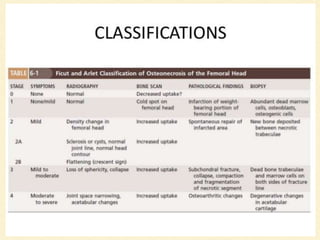
Ficat and ArletClassification
Steinberg Classification
The Association Research Circulation Osseous (ARCO)
system
Japanese Orthopaedics Association (Ohzono)
CORE DECOMPRESSION
Treatment ofchoice for
Ficat and Arlet I,IIA
reversible etiology
Simple to perform , very low complication
More effective than nonoperative treatment of early
Osteonecrosis of femoral head
40.
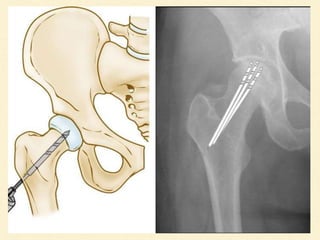
CORE DECOMPRESSION
Reduce theintraosseus pressure in the femoral head
Restore Normal vascular flow
Subsequently alleviate the pain in the hip
COMPLICATION
The natural historyof AVN involves subchondral necrosis ,
subchondral fracture and collapse of bone, deformity of the
articular surface , and osteoarthritis
In later stages, sclerosis and total destruction of the joint
may occur
Nonunion of fracture and secondary muscle wasting are
potential complications