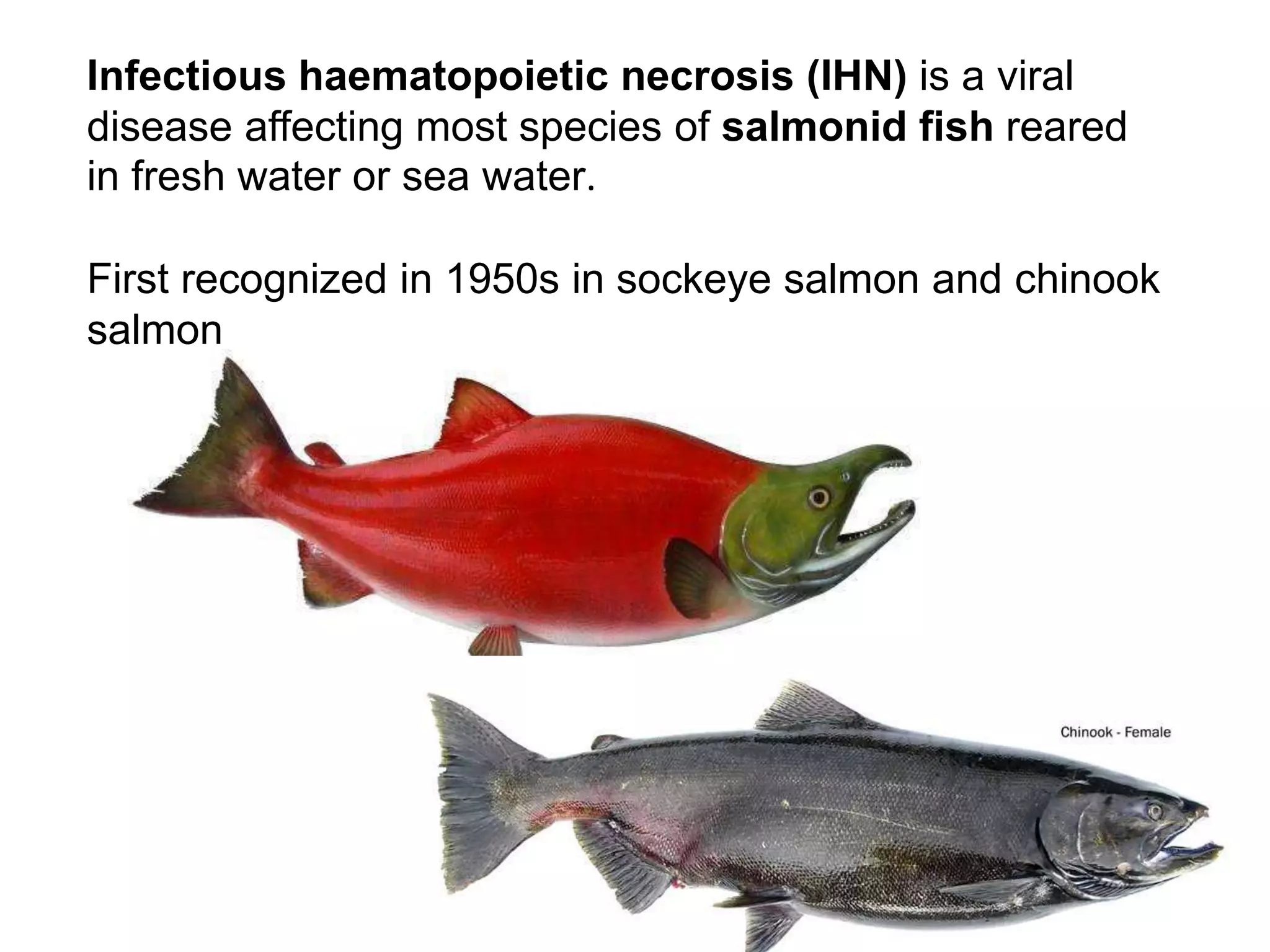
This document summarizes information about infectious haematopoietic necrosis (IHN), a viral disease affecting salmonid fish. IHN is caused by the fish rhabdovirus IHNV. It primarily affects rainbow trout farms, where it can cause high mortality rates in acute outbreaks. IHNV has a single-stranded RNA genome and infects hematopoietic tissues like the kidney and spleen. Clinical signs include darkening of the skin, exophthalmia, and hemorrhaging. Diagnosis involves examining tissue imprints for necrobiotic bodies and detecting the virus through electron microscopy, which reveals bullet-shaped virions in infected cells.
















































































































![CCleaner Professional Key v6.25.11093 with Crack Download [Latest ]](https://cdn.slidesharecdn.com/ss_thumbnails/fishviraldiseasespresentation-250629164253-73b1e46f-thumbnail.jpg?width=640&height=640&fit=bounds)

















































