Downloaded 73 times












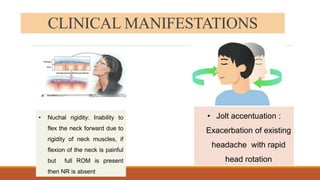










This document provides information on meningitis, including: - Meningitis is an inflammation of the meninges (membranes covering the brain and spinal cord) that can be caused by bacteria, viruses, fungi, or other causes. - Common symptoms include fever, headache, and neck stiffness. - Bacterial meningitis requires immediate treatment with antibiotics to prevent disability or death. Viral meningitis is generally less severe but still requires supportive care. - Complications can include hearing loss, seizures, learning difficulties, and even death if not properly treated.






















































![Human genome project [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/humangenomeprojectautosaved-210929062307-thumbnail.jpg?width=640&height=640&fit=bounds)
































