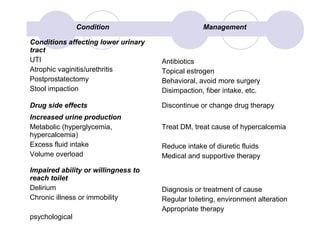
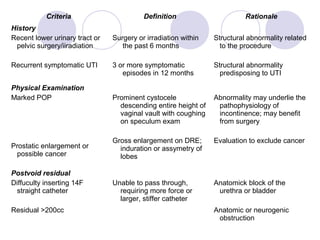
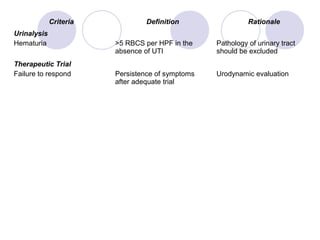

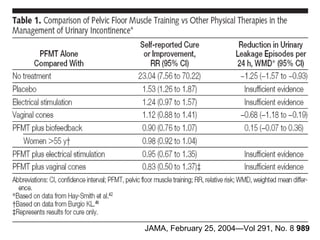


This document discusses urinary incontinence in the elderly. It defines incontinence and notes that its prevalence increases with age, affecting more women than men. Types of incontinence include stress, urge, overflow, and functional. Evaluation involves history, exam, urinalysis and residual urine measurement to identify reversible causes and guide management. Management includes behavioral techniques, drug therapy, surgery, and catheters depending on the underlying causes. Pelvic floor muscle training and prompted voiding are effective non-drug interventions for some patients.























































































