The document provides an overview of incomplete spinal cord injuries. Some key points:
- Spinal cord injuries can range from complete to incomplete, depending on the severity and location of the lesion in the spinal cord. Incomplete injuries result in partial preservation of motor or sensory function below the injury level.
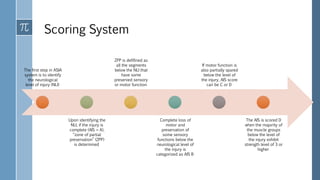
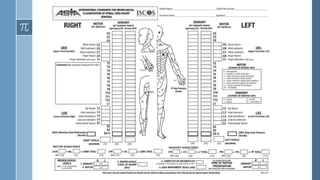
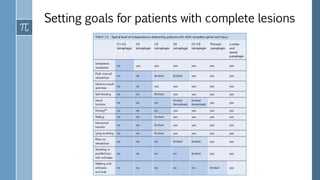
- The American Spinal Injury Association (ASIA) scoring system is used to clinically classify spinal cord injuries based on motor and sensory function. Injuries are classified on a scale from A (complete injury) to D (near normal function).
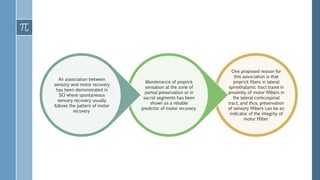
- Recovery from incomplete injuries is possible, though most occurs within the first year as spontaneous recovery plateaus. Sensory preservation is a predictor of potential motor recovery.















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



