Downloaded 633 times

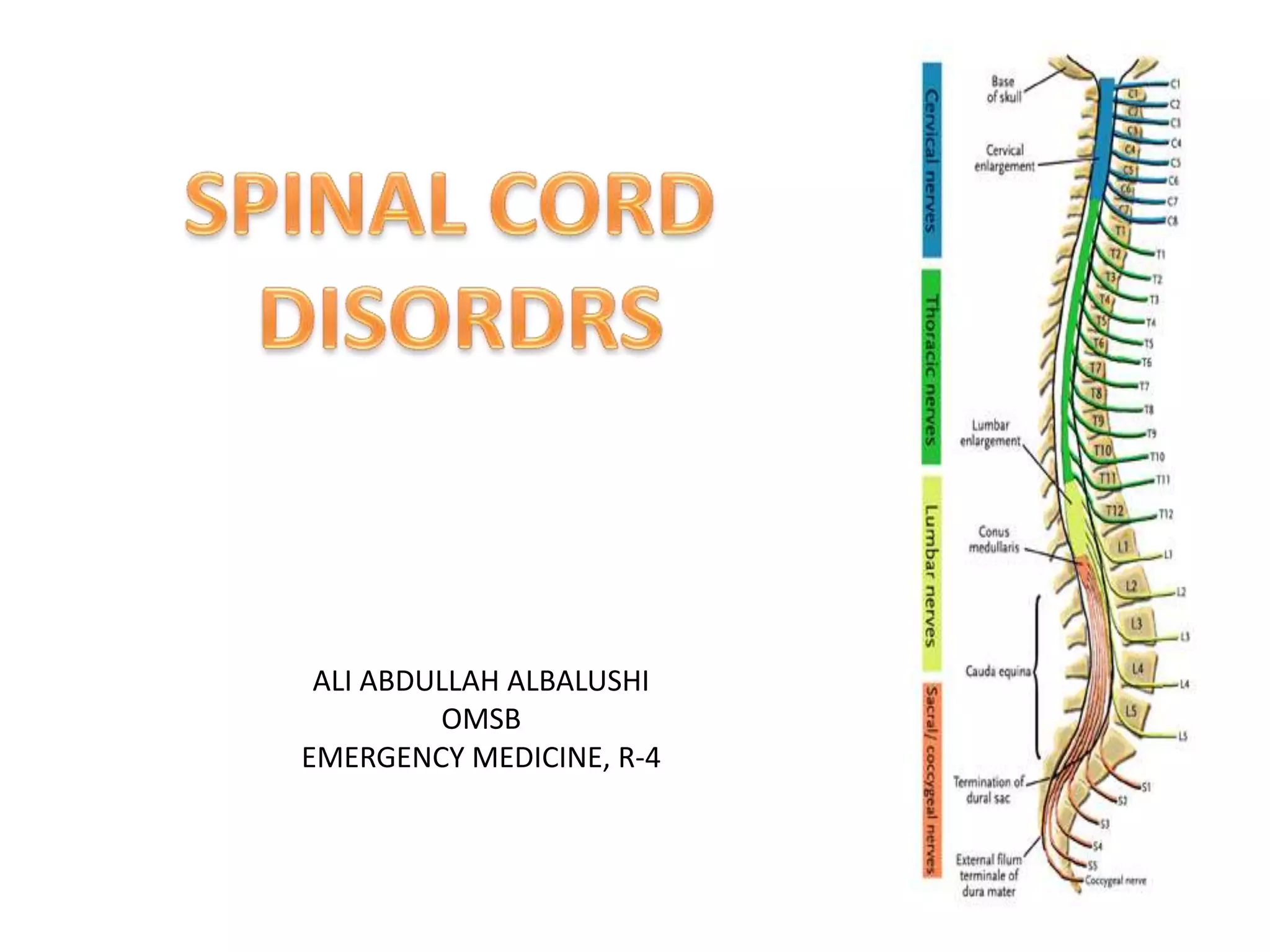
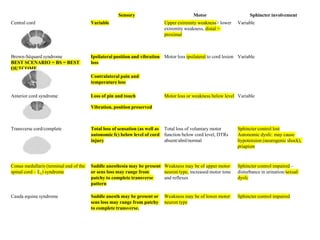
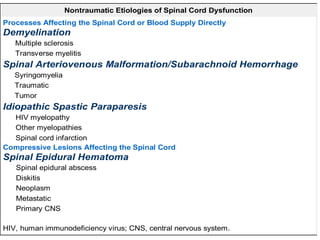


This document discusses spinal cord disorders and provides information on spinal cord anatomy and different types of spinal cord injuries and conditions. It outlines 15 questions regarding the anatomy of the spinal cord and characteristics of various spinal cord disorders including central cord syndrome, Brown-Sequard syndrome, anterior cord syndrome, transverse myelitis, syringomyelia, spinal epidural hematoma, spinal epidural abscess, diskitis, and spinal cord neoplasms. The document seeks to test the reader's knowledge on the topics covered through true or false questions.























































































