Downloaded 196 times

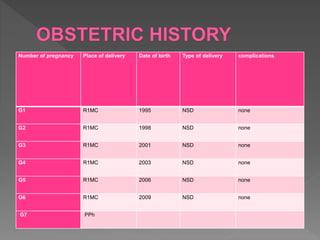
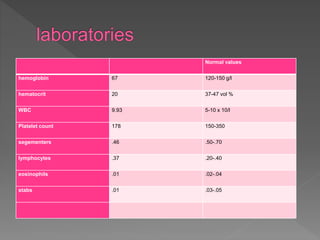







Patient BM, a 39 year old female, presented with heavy vaginal bleeding, abdominal pain and fever for the past 3 days. She was 7 4/7 weeks pregnant. Her symptoms were consistent with an incomplete abortion. She underwent dilatation and curettage to complete the evacuation of the pregnancy remains in the uterus. Her bleeding was thought to be due to an incomplete abortion and not induced or associated with infection. Blood transfusion and antibiotics were provided due to signs of anemia and fever.























































































