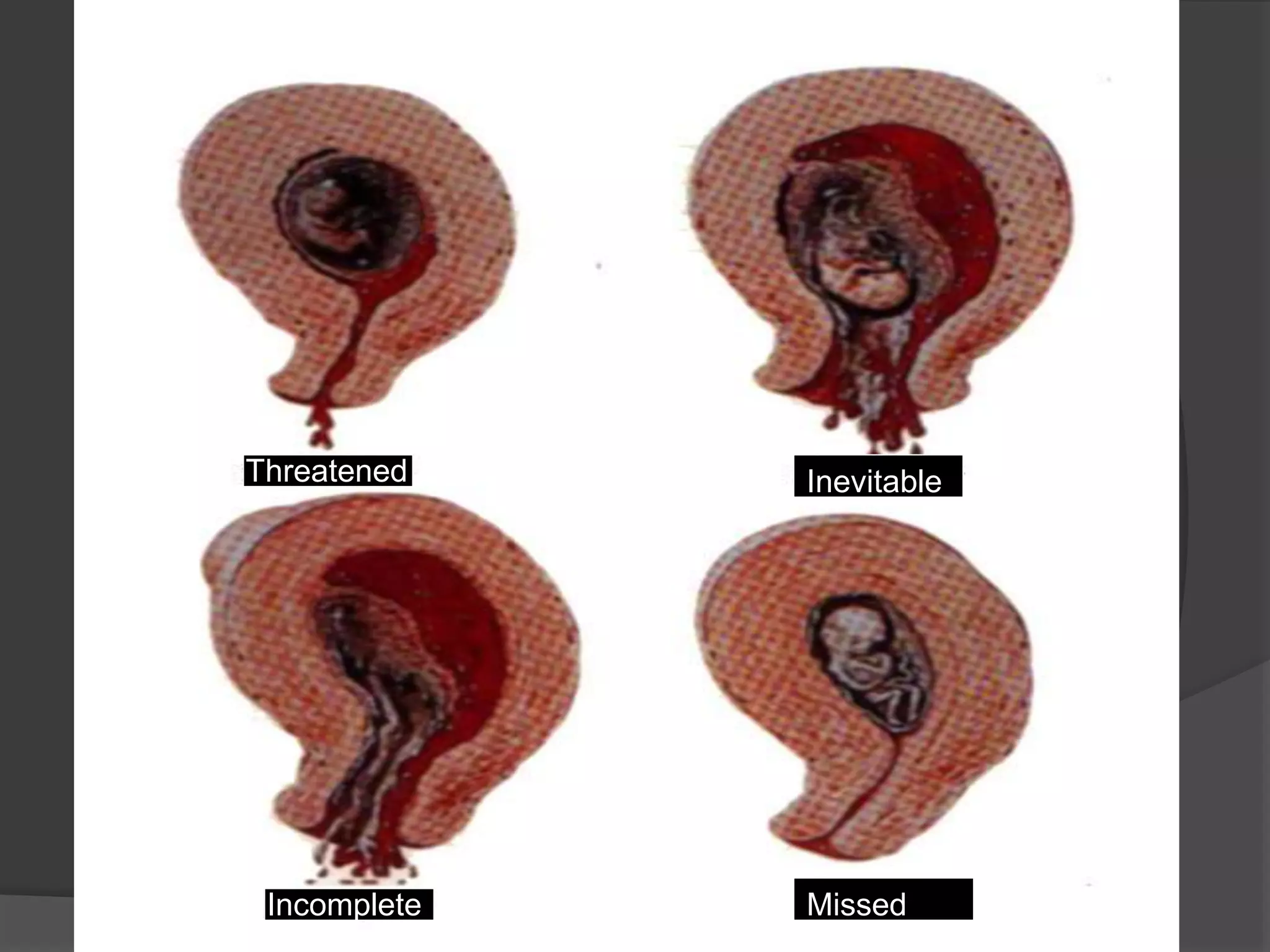
This document defines abortion and describes the different types, including spontaneous (threatened, missed, inevitable, etc.) and induced (therapeutic, criminal). It discusses the causes, signs and symptoms, and general management of abortion. Spontaneous abortion is commonly referred to as miscarriage and can be threatened, missed, inevitable complete or incomplete. Induced abortion can be therapeutic when performed by a doctor for medical reasons, or criminal when illegally procured. Management involves determining the cause, preserving the mother's life, and preparing for future pregnancies.