Downloaded 47 times
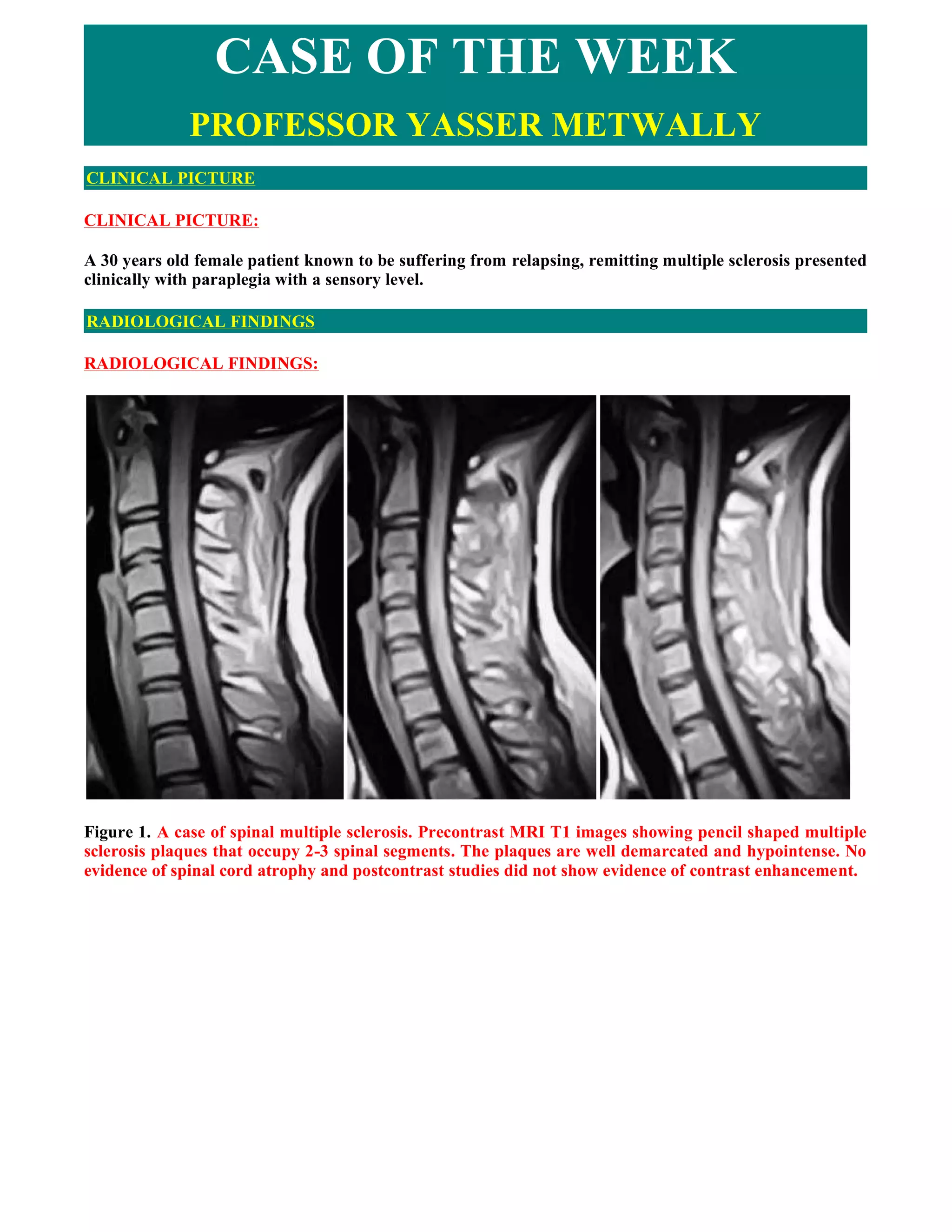
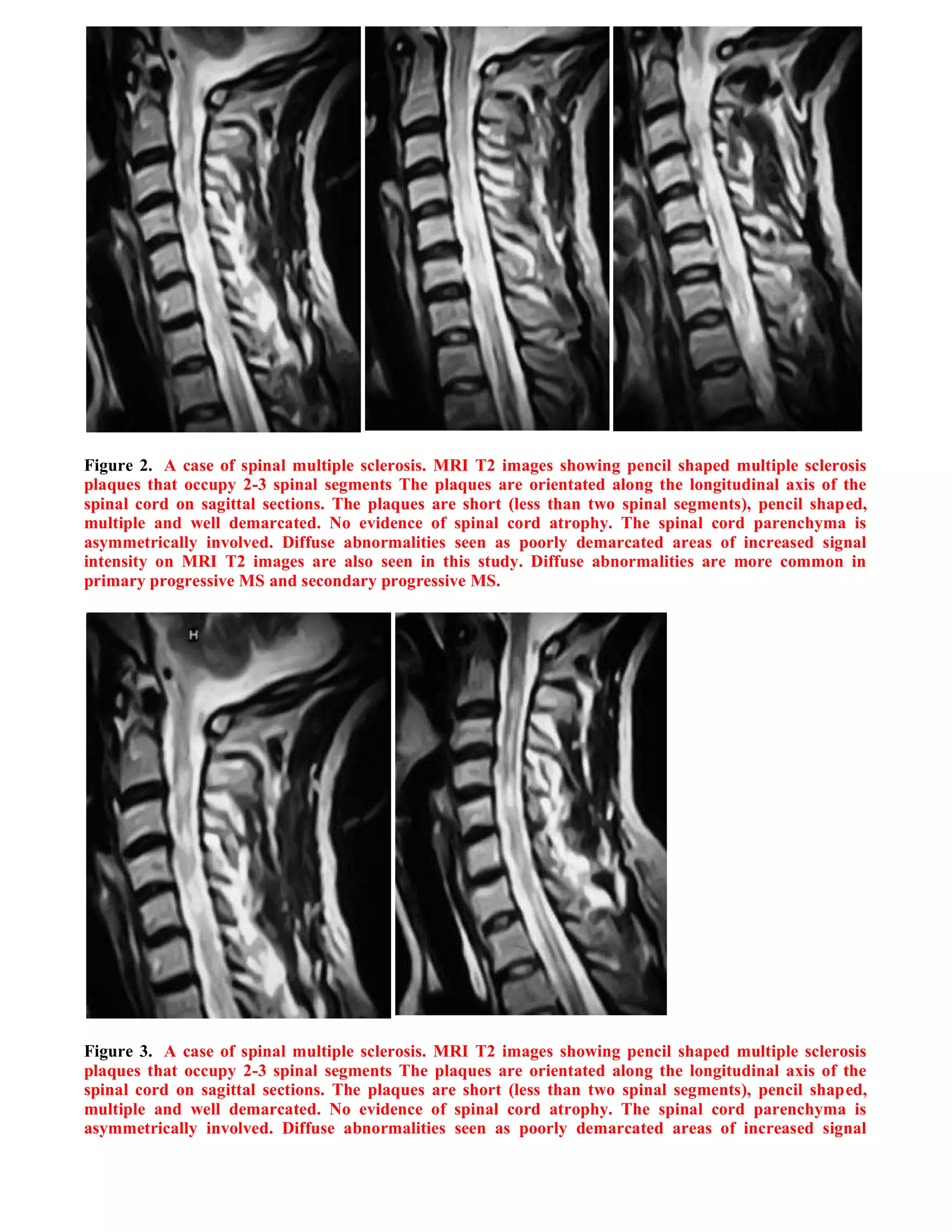
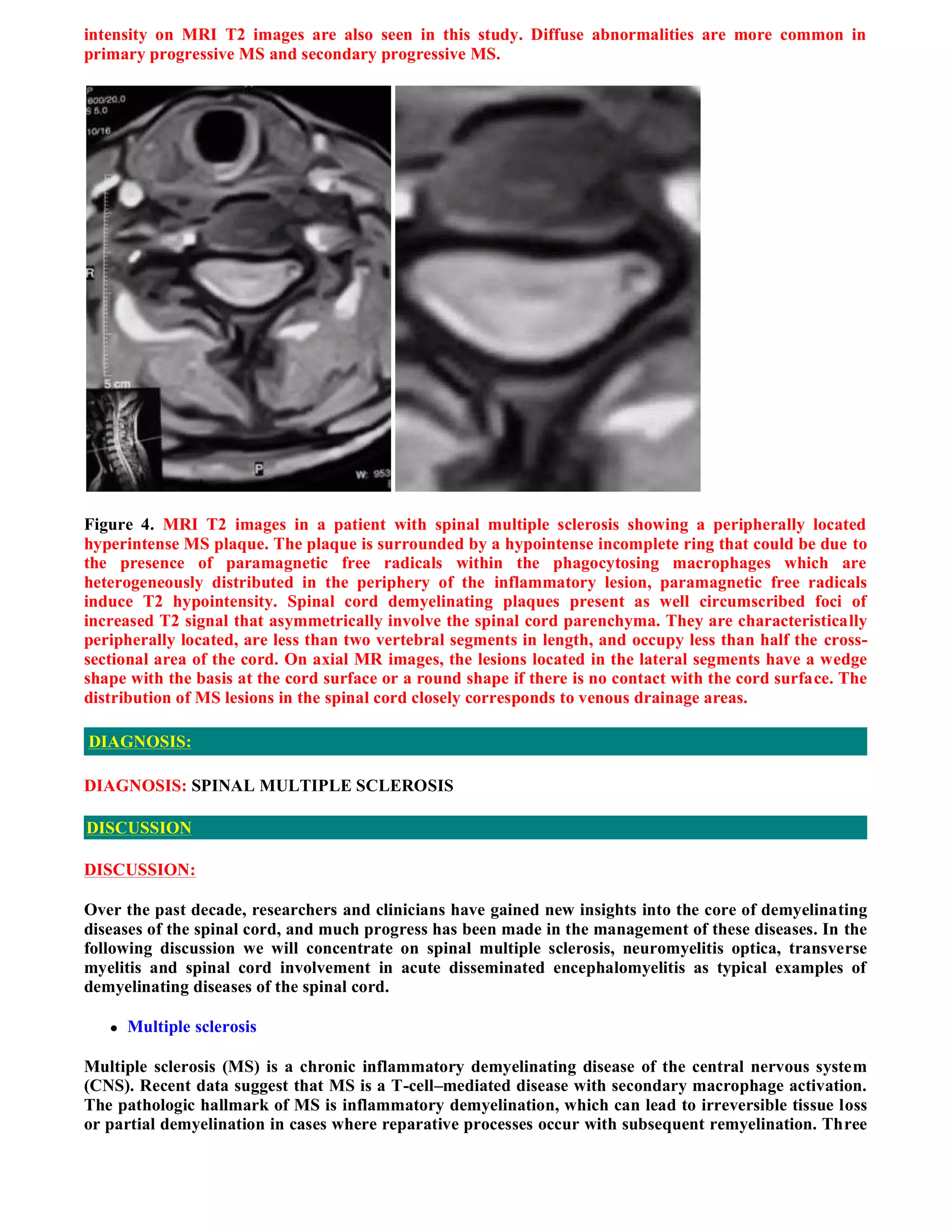

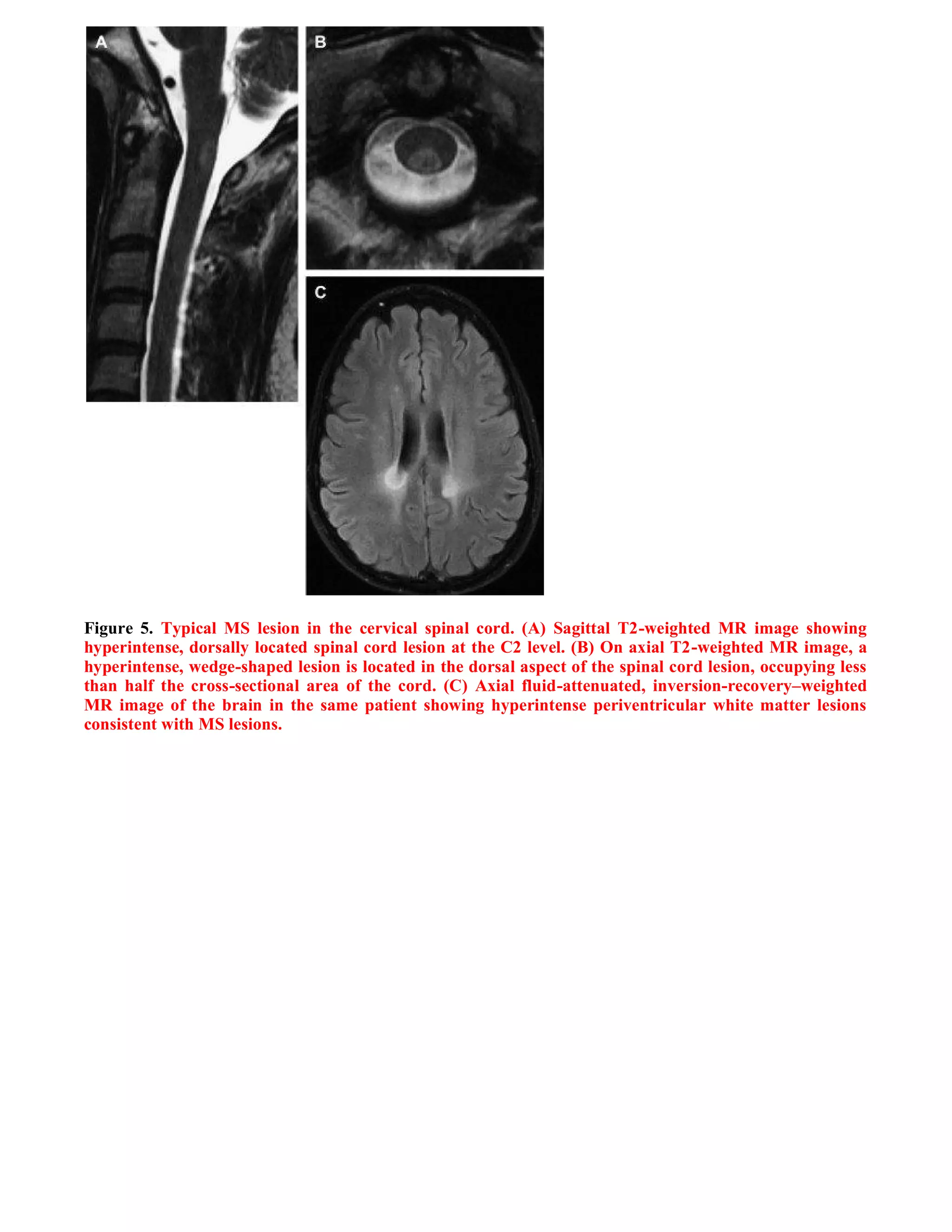

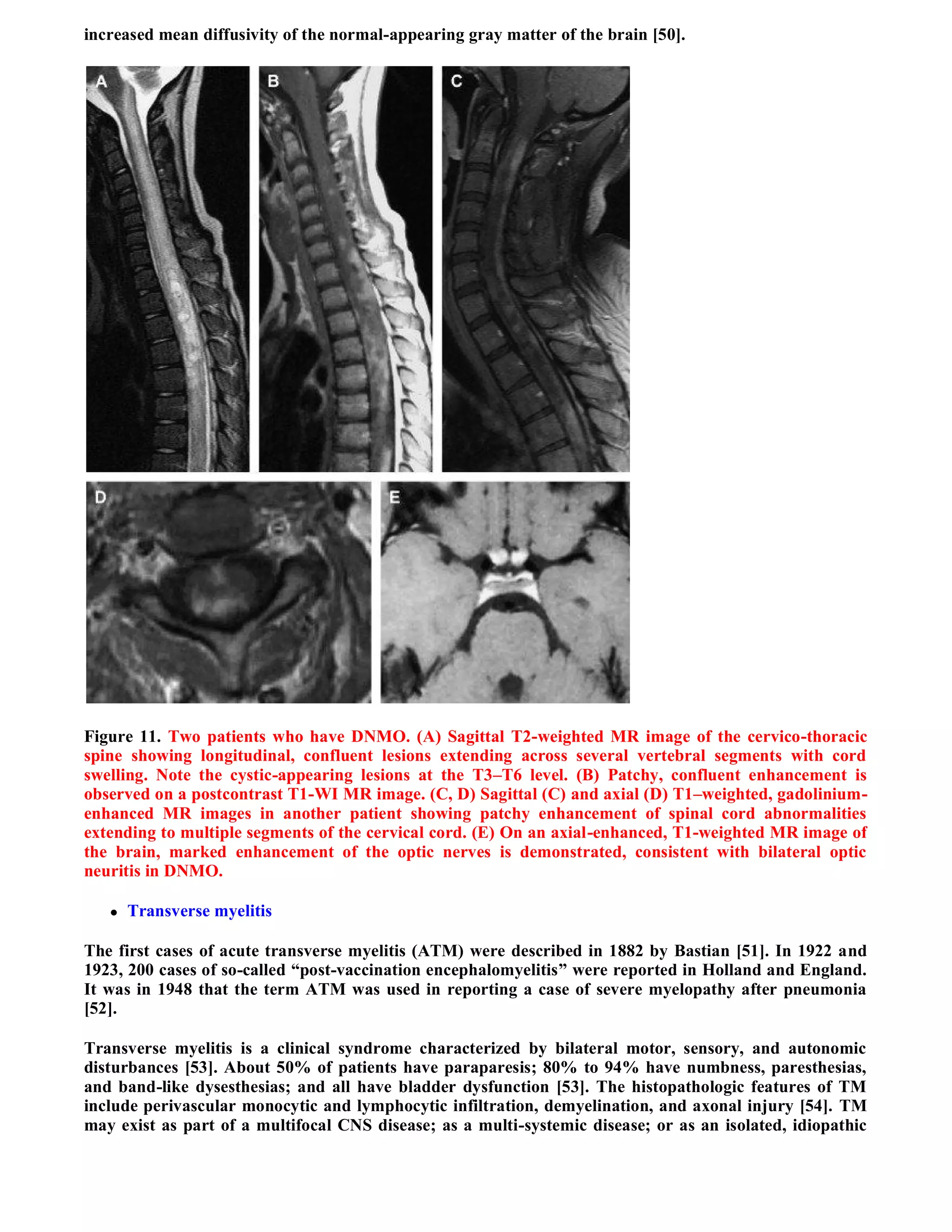
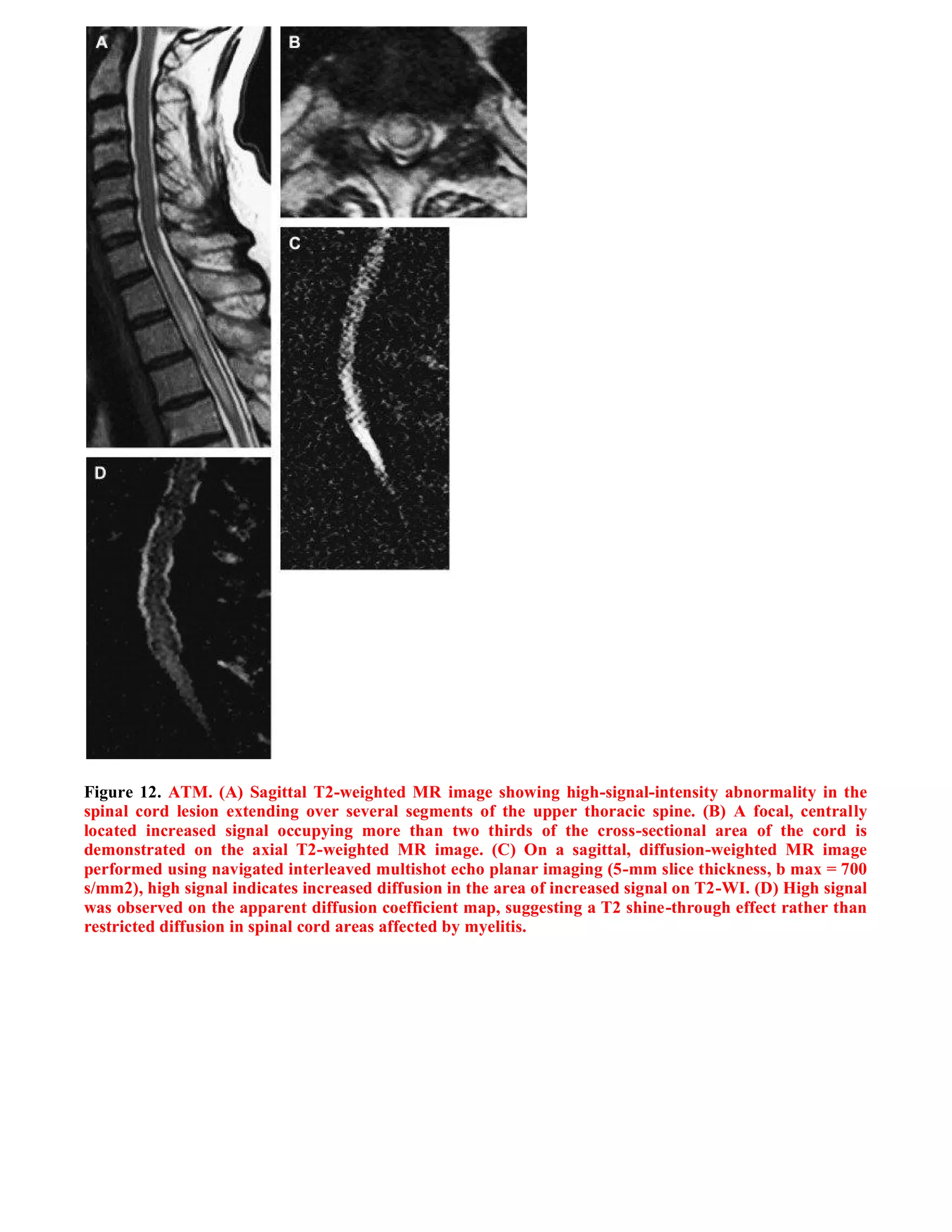

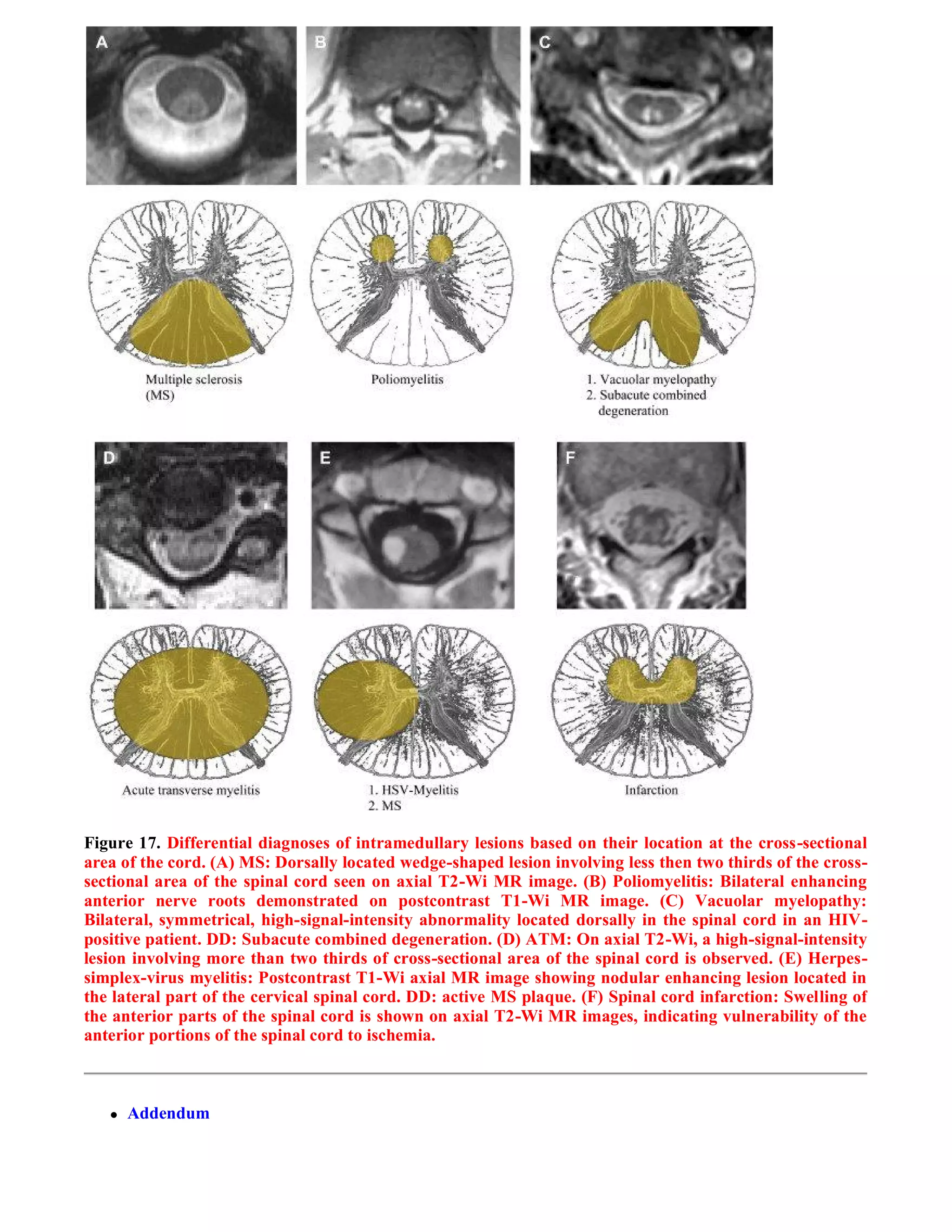

This document summarizes a case study of spinal multiple sclerosis seen on MRI imaging. It includes the following key points: 1) MRI images of the patient show multiple well-defined pencil-shaped lesions occupying 2-3 spinal segments that appear hypointense on T1-weighted images and hyperintense on T2-weighted images. 2) The lesions are characteristic of multiple sclerosis and located peripherally within the spinal cord. 3) The imaging and clinical presentation lead to a diagnosis of spinal multiple sclerosis.










































































































