Downloaded 13 times





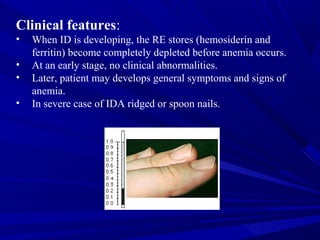






This document discusses classification and causes of anemia, focusing on iron deficiency anemia. It describes the normal iron metabolism process and requirements. Causes of iron deficiency anemia include blood loss, insufficient dietary iron intake, and malabsorption. Laboratory findings of iron deficiency anemia show a low hemoglobin with decreased MCV, MCH, and MCHC, known as a hypochromic microcytic blood film. The bone marrow appears hypercellular with increased red blood cell precursors that stain negative for iron.















































































![Skin anatomy chc training 2012 [compatibility mode] [repaired]](https://cdn.slidesharecdn.com/ss_thumbnails/skinanatomychctraining2012compatibilitymoderepaired-131009014235-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)





