Downloaded 28 times

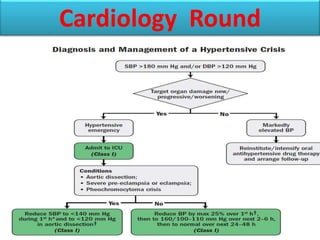
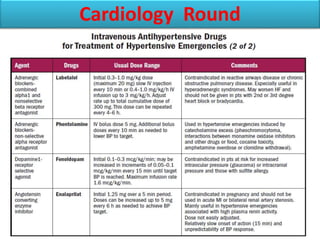
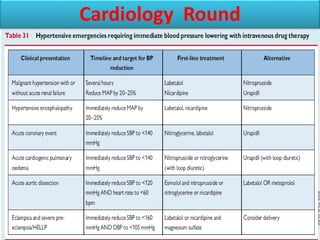
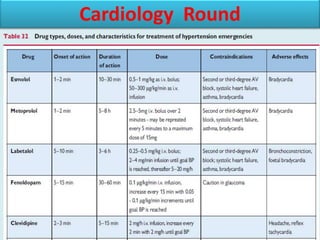
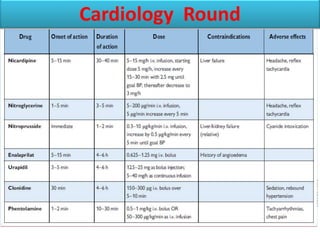

A 45-year-old man presented with headache, visual disturbances, and papilledema with a blood pressure of 200/115 mmHg. He was admitted to the CCU/ICU. This case represents a hypertensive emergency characterized by severe hypertension (grade 3) associated with acute hypertensive emergency organ damage (HMOD) including papilledema, which requires immediate but careful intervention to lower blood pressure, usually with intravenous therapy. Hypertensive emergencies typically present with severe hypertension, funduscopic changes, microangiopathy, and can be associated with encephalopathy, acute heart failure, and acute renal deterioration. The goal of treatment is to reduce blood pressure to prevent further organ damage.








































![Hypertensive Crisis diagnosis treatment [1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypertensivecrisis1-241128145637-9d731b1a-thumbnail.jpg?width=640&height=640&fit=bounds)














































