Download as PPSX, PPTX
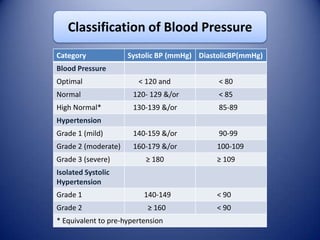
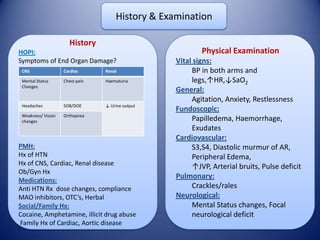
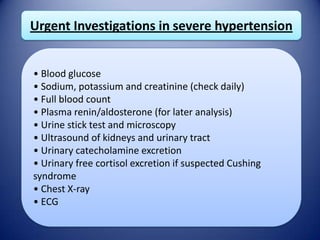
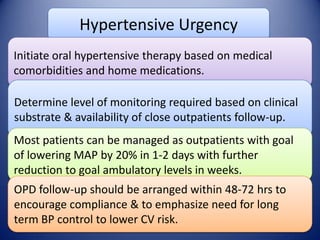

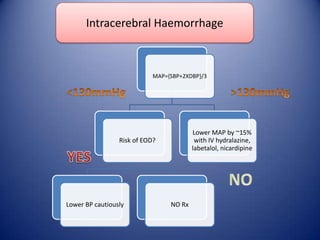


This document provides information on hypertensive emergencies and urgencies, including their classification, evaluation, and management. It defines hypertensive emergencies as severe hypertension with evidence of acute target organ damage, while urgencies involve severe hypertension without organ damage. For emergencies, rapid parenteral treatment is needed to stop organ damage progression while avoiding hypoperfusion. Several parenteral agents are discussed for specific conditions along with their dosing and side effects. The goal is to lower blood pressure gradually to avoid complications. Hypertensive urgencies can often be treated orally as outpatients after initial control.










































































































