Downloaded 268 times
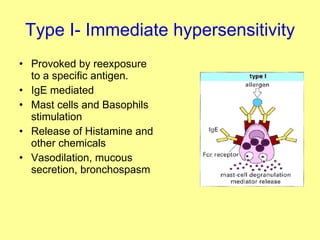
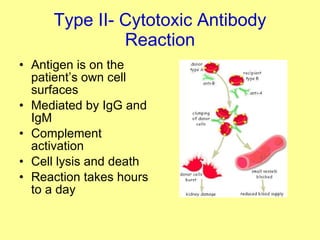

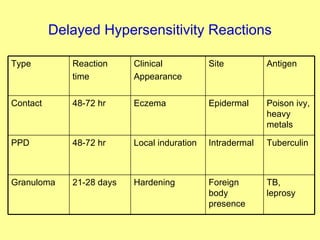
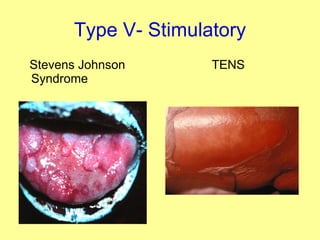



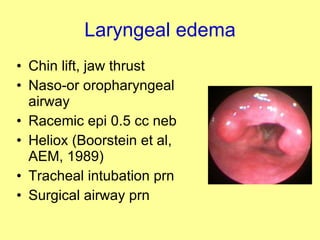

This document provides an overview of the different types of hypersensitivity reactions. It describes the pathophysiology, clinical manifestations, treatments, and examples for each of the 5 types of hypersensitivity reactions: Type I (immediate/anaphylactic), Type II (cytotoxic antibody), Type III (immune complex), Type IV (delayed-type), and Type V (stimulatory). It also provides details on the diagnosis and management of anaphylaxis, including the use of epinephrine as first-line treatment.























































































