Downloaded 37 times





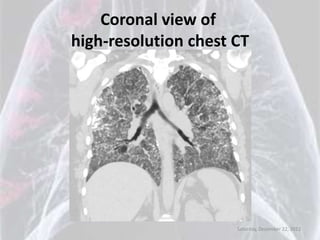

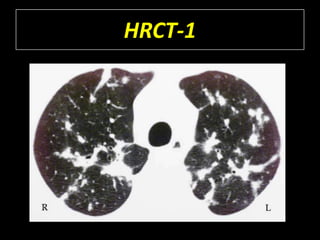
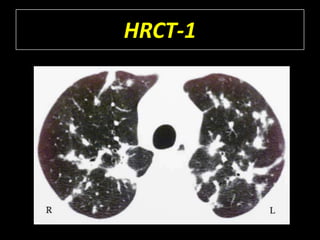
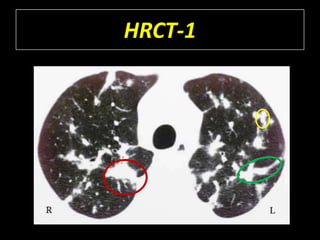
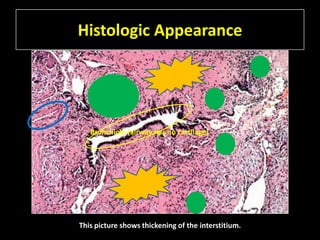



The abnormality seen on this HRCT image is predominantly subpleural and basal. There are bilateral reticular opacities in the subpleural regions extending into the bases posteriorly. The lung apices and upper lobes appear relatively spared.