Downloaded 13 times






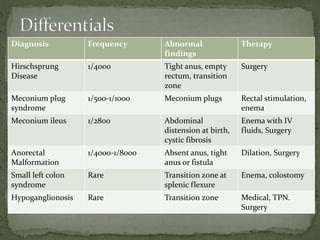
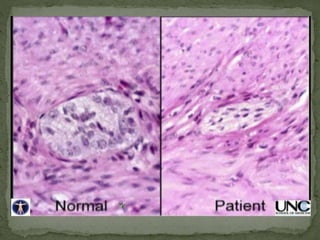
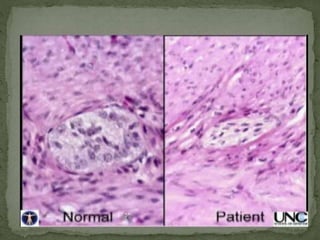
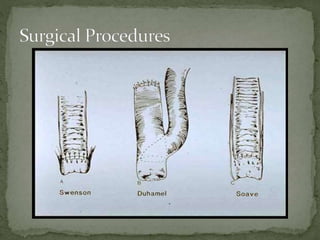

This document discusses the case of a 2-month-old baby girl presenting with vomiting, abdominal distension, and failure to pass meconium. Imaging showed dilated bowel loops. A barium enema suggested Hirschsprung's disease or constipation. Biopsies during exploratory surgery confirmed Hirschsprung's disease. The baby later underwent a Soave endorectal pull-through procedure to correct the condition. The document also reviews the differential diagnosis, diagnostic testing, molecular basis, surgical treatment options, and postoperative management of Hirschsprung's disease.



































































