Hirschsprung's disease by dr abhinav kesarwani
•Download as PPTX, PDF•
13 likes•887 views

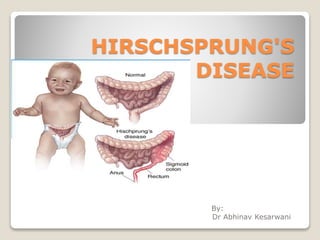
Hirschsprung's disease is a congenital condition where the distal segments of the intestinal tract lack intrinsic ganglion cells. This causes mechanical obstruction due to failure of the affected areas to relax during peristalsis. It most commonly affects the rectum and sigmoid colon. The diagnosis is established through a combination of clinical presentation, radiological imaging like barium enema, rectal biopsy, and manometry. Treatment involves initial decompression and colostomy followed by a definitive pull-through surgery like Swenson or Soave procedure to remove the aganglionic segment. Complications can include anastomotic leak, postoperative enterocolitis, constipation and incontinence.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Hirschsprung's disease by dr abhinav kesarwani
Similar to Hirschsprung's disease by dr abhinav kesarwani (20)
Recently uploaded
Recently uploaded (20)
Hirschsprung's disease by dr abhinav kesarwani
- 2. It was first described in 1888 by Harald Hirschsprung (1830-1916): paediatrician, Denmark
- 3. INTRODUCTION Hirschsprung's disease (HD) is a congenital disease in which there is a lack of intrinsic nerves (ganglion cells) in the distal segments of the intestinal tract. These abnormal segments produce mechanical obstruction because of failure to relax during peristalsis. Hirschsprung's disease always starts in the anal verge, but the length of the segment without ganglion cells (aganglionic) varies: it is limited to the rectum and sigmoid in 75% of patients; involves the whole colon in 8%; and rarely involves the small bowel. The incidence of Hirschsprung's disease varies from 1 in 5,000 to 1 in 10,000 live births. The diagnosis is established in 15% within the first month of life, in 40-50% in the first 3 months, in 60% at the end of the first year of age, and in 85% by 4 years.
- 5. During normal fetal development cells from neural crest migrate into the large intestine to form the network of nerves called Auerbach’s plexus (Muscularis externa) and Meissner’s plexus ( submucosa) -Occurs in the end of first trimester -Lack of these nerves causes failure of relaxation of the involved part of the colon. -Also supplied by sympathetic nerves, and intrinsic component (enteric nervous system) Embryology
- 6. HD, due to failure of neural crest cells to migrate caudally Aganglionosis begins at anorectal line (internal anal sphincter)
- 7. Types 1. Congenital : Commonest Etiology of the disease is still unknown but Genetic factors are now identified(10th chromosome, RET-protooncogene, Endothelin B gene) 10% of cases have familial history, especially those with long segment disease. 2. Acquired : ◦ Degeneration of the ganglions may occur due to: -Vascular causes like after pullthrough procedure due to ischemia & tension. - Non vascular causes like ◦ Trypanosoma (chaga's disease). ◦ Vit B1 def. ◦ Chronic infection(TB).
- 8. Presentation In newborns -95% Failure to pass meconium in first 24hrs life -Abdomen distension -Vomiting (bilious) -Constipation or gas -Diarrhoea In older children -Chronic constipation -Abdomen distention -Failure to thrive -10-15% - severe diarrhea alternating with constipation— enterocolitis of Hirschsprung’s disease
- 9. Associated disorders Associated anomalies do occur in nearly 20% of cases Down’s Syndrome(5-15%) Urogenital Abnormalities Cardiovascular Abnormalities Congenital deafness Malrotation, Gastric diverticulum or Intestinal atresia Waardeberg Syndrome
- 10. Waardeberg syndrome An inherited auotosomal dominant disorder -hearing loss -Pigmented anomalies affecting the eyes, hair, skin and various defects of neural crest derived tissues
- 11. Diagnosis History: failure to pass meconium, painless abdomen distension & constipation) Physical examinations: Distended abdomen with Multiple fecal masses on abdominal examination On Rectal Examination characteristically there is Hypertonic Anal sphincter Rectum is typically empty. Hard fecal mass.
- 12. Radiology 1. Plain x-rays of the abdomen : Erect & supine 2. Contrast Enema. Shows narrow distal segment, funnel-shaped dilatation at level of transition zone with marked dilatation of the proximal colon. 24-hrs delayed films is important in diagnosis; it shows poor emptying with barium throughout the colon, as opposed to the child with psychogenic stool holding in whom the barium generally collects in the distal rectosigmoid.
- 14. Barium Enema -Less sensitive for detecting short lesions, total colon aganglionosis, and disease of the newborn -Many newborns do NOT show definitive transition zone -Delayed evacuation of contrast
- 17. Electromanometry: -The classic finding is the absence of the recto anal inhibitory reflex when the rectum is distended. (Lack of internal anal sphincter relaxation in response to rectal stretch), ballooning -not useful in neonate -excellent screening tool in infant & children Rectal biopsy : -Definitive diagnostic test -demonstrates absence of ganglion cells, nerve hypertrophy and stains indicating increased acetylcholinesterase activity. -Suction mucosal biopsy (at different levels ), can be done without anesthesia -Full thickness biopsy is done under general anesthesia. UltraSonography: for associated anomalies.
- 19. Treatment -Decompression: introduce a rectal tube and irrigation -Colostomy -Definitive procedures -Closing of the stoma
- 20. Management Acute I.O. -NGT , -IVF , -Antibiotics , -Rectal tube irrigations . -The initial treatment requires performing a colostomy. ( multiple seromuscular biopsies) Note: The colostomy is placed above the transition zone. Placement in an area of aganglionosis will lead to persistent obstruction. Definitive treatment will be planned. Chronic constipation : -Laxative -Saline enema. -Work up to establish the diagnosis -Definitive treatment will be planned
- 21. Definitive Procecdures By the age of 6-12 months; 9kg or more), a formal pull- through procedure is done 1) Open surgery : There are many surgical options for Pull-through operation. All aiming at resection of aganglionic segment They give excellent result in 90%. a. Swenson b. Soave c. Rehbein d. Duhamel e. Boley's
- 22. Swenson Procedure -Sharp extrarectal dissection down to 2 cm above the anal canal -Aganglionic colonic segment resected -End-to-end anastamosis of normal proximal colon to anal canal -Completely removes defective aganglionic colon
- 23. Duhamel Procedure -Posterior portion of defective colon segment resected -Side to side anastamosis to left over portion of rectum -Constipation a major problem due to remaining aganglionic tissue. -Simpler operation, less dissection.
- 24. Soave Procedure Circumferential cut through muscular coat of colon at peritoneal reflection Mucosa separated from the muscular coat down to the anal canal Proximal normal colon is pulled through retained muscular sleeve Telescoping anastamosis of normal colon to anal canal. Advantage: rectal intramural dissection ensures no damage to pelvic neural structures Higher rate enterocolitis, diarrhoea, often requires repeated dilations
- 25. Overall Mortality: -Swenson procedure: 1-5% -Duhamel procedure: 6% -Soave procedure: 4-5% Operative Complications -Leak at anastamosis: 5-7% -Postop Enterocolitis: 19-27% -Constipation -Stricture Formation -Incontinence
- 26. 2) LAPAROSCOPY: Transanal endorectal pullthrough -Excised aganglionic tissues removed through anal canal -no abdominal incision -Better results in terms of pain, return of bowel function, shortens hospital stay -Similar incidence of leaks, pelvic abscesses, enterocolitis.
- 29. One vs Two Stage procedure Early complications: No difference in incidence of anastomotic leak, pelvic infection, prolonged ileus, wound infection, wound dehiscence Late complications: No difference in incidence of anastomonic stricture, late obstruction, constipation, incontinence, urgency Postoperative enterocolitis higher in 1 stage (42% vs 22%)
- 31. Thank you