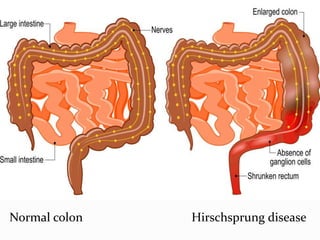
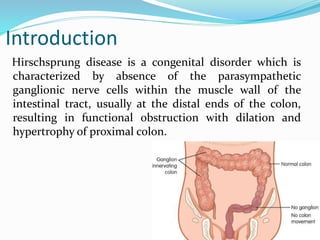
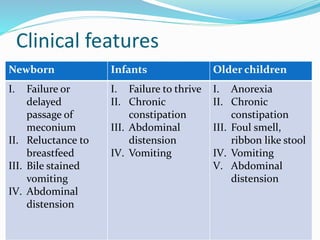
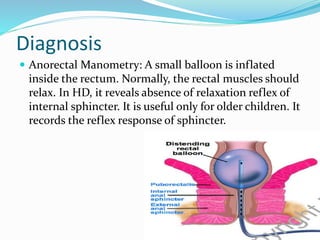
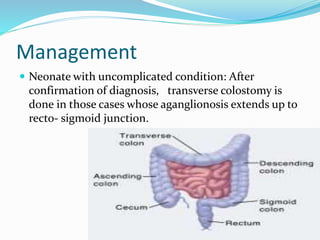
This document provides an overview of Hirschsprung disease, including its incidence, etiology, pathophysiology, clinical features, diagnosis, management, nursing management, and complications. It describes Hirschsprung disease as a congenital disorder characterized by the absence of ganglion cells in parts of the colon, most commonly in the rectum and sigmoid colon. The document discusses the various levels of Hirschsprung disease, clinical presentation in newborns and older children, diagnostic tests, surgical treatments including colostomy and pull-through procedures, nursing care both pre-and post-operatively, and potential complications.