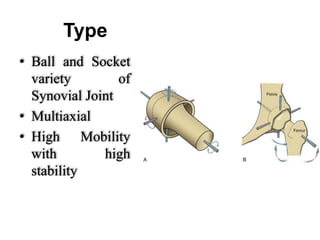
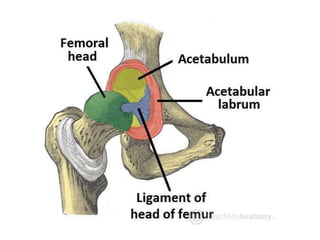
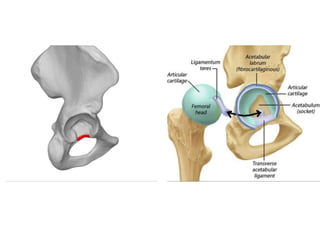

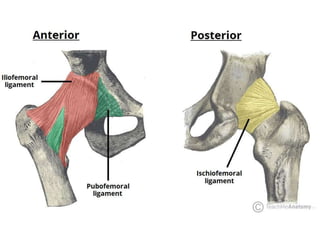
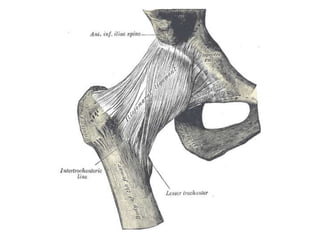
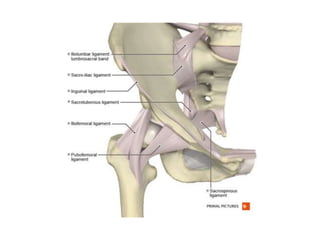
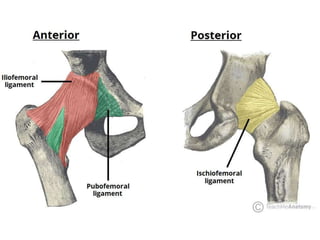
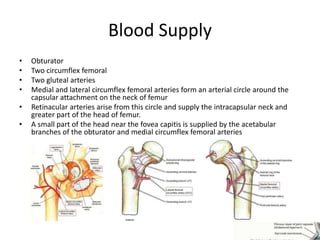

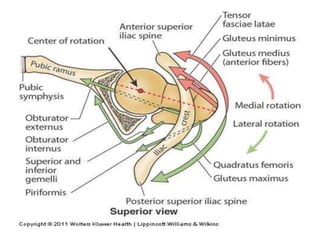
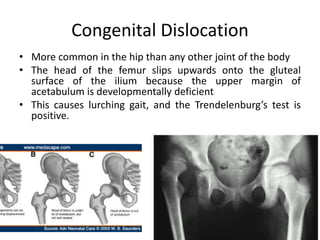
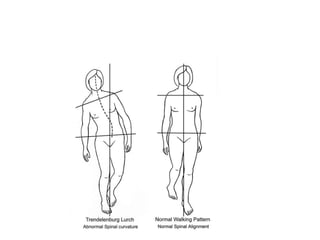
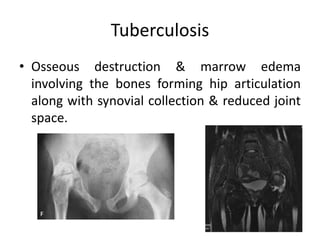
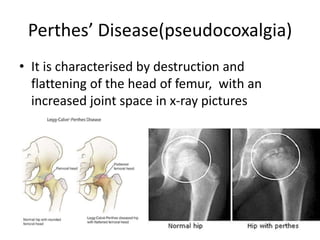
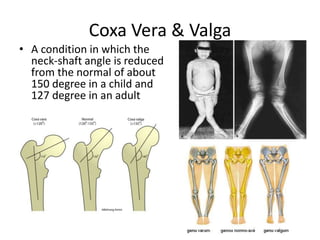
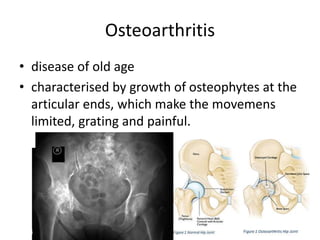

The hip joint is a ball and socket synovial joint that allows high mobility. It has an articular femoral head that fits into the acetabulum of the hip bone. Strong ligaments like the iliofemoral ligament provide stability. Blood is supplied by various arteries and it is innervated by nerves from the lumbar and sacral plexuses. Common conditions affecting the hip joint include congenital dislocation, Legg-Calve-Perthes disease, osteoarthritis, and fractures of the femoral neck.























































































