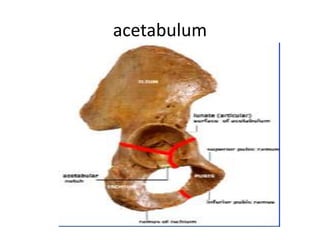
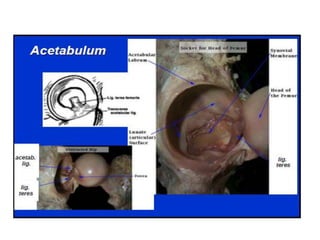
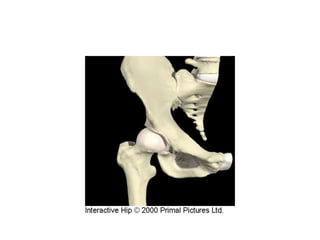
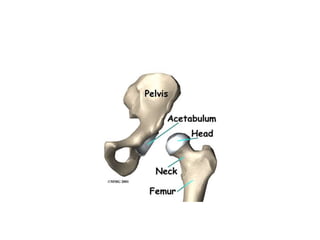
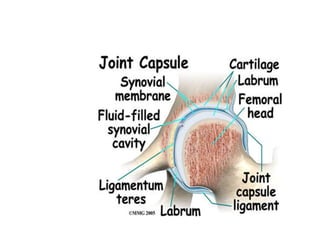
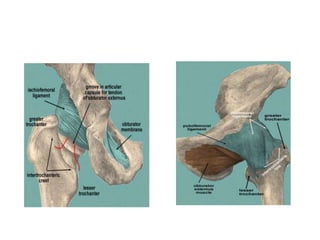
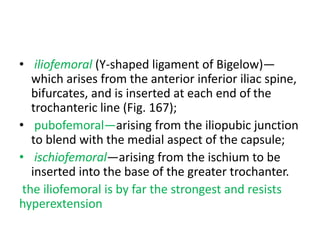
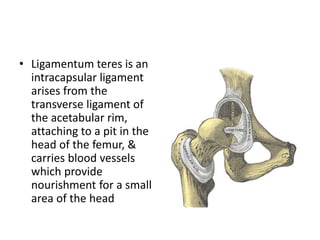
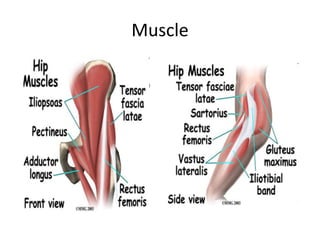
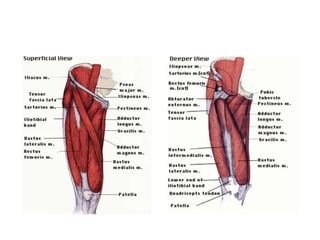
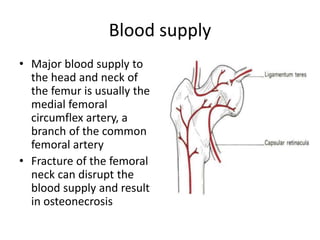
The hip joint is a ball-and-socket joint between the femur and acetabulum. It is made up of bones, cartilage, ligaments, synovial membrane, muscles and nerves. The acetabulum forms the socket of the joint and is reinforced by the acetabular labrum. The femoral head forms the ball and articulates with the acetabulum. Strong ligaments including the iliofemoral, ischiofemoral and pubofemoral ligaments reinforce the joint capsule. The hip joint is supplied by branches of the femoral, sciatic and obturator nerves and has an extensive blood supply. Bursae around the hip joint help with movement.