Download as PDF, PPTX



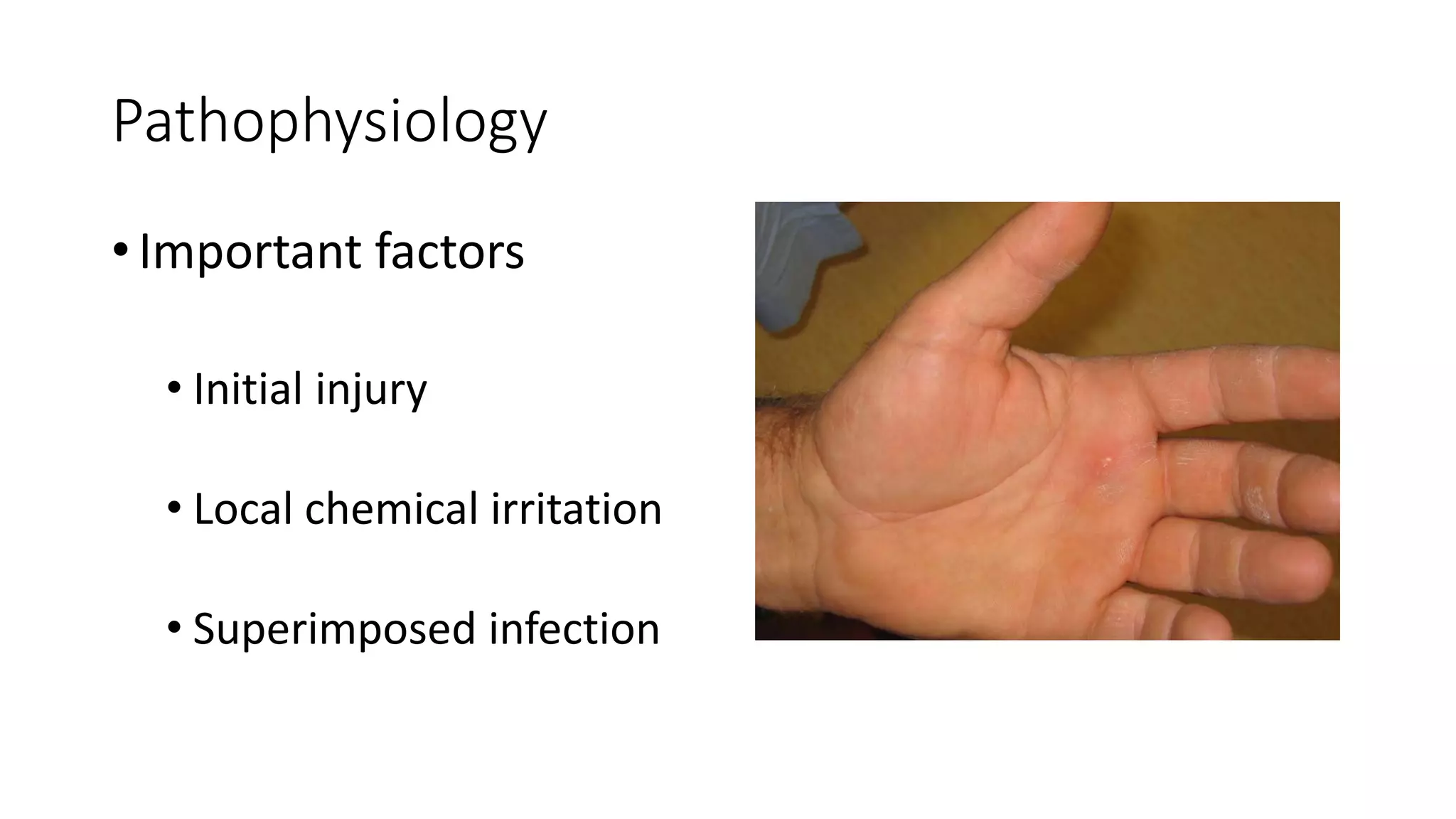

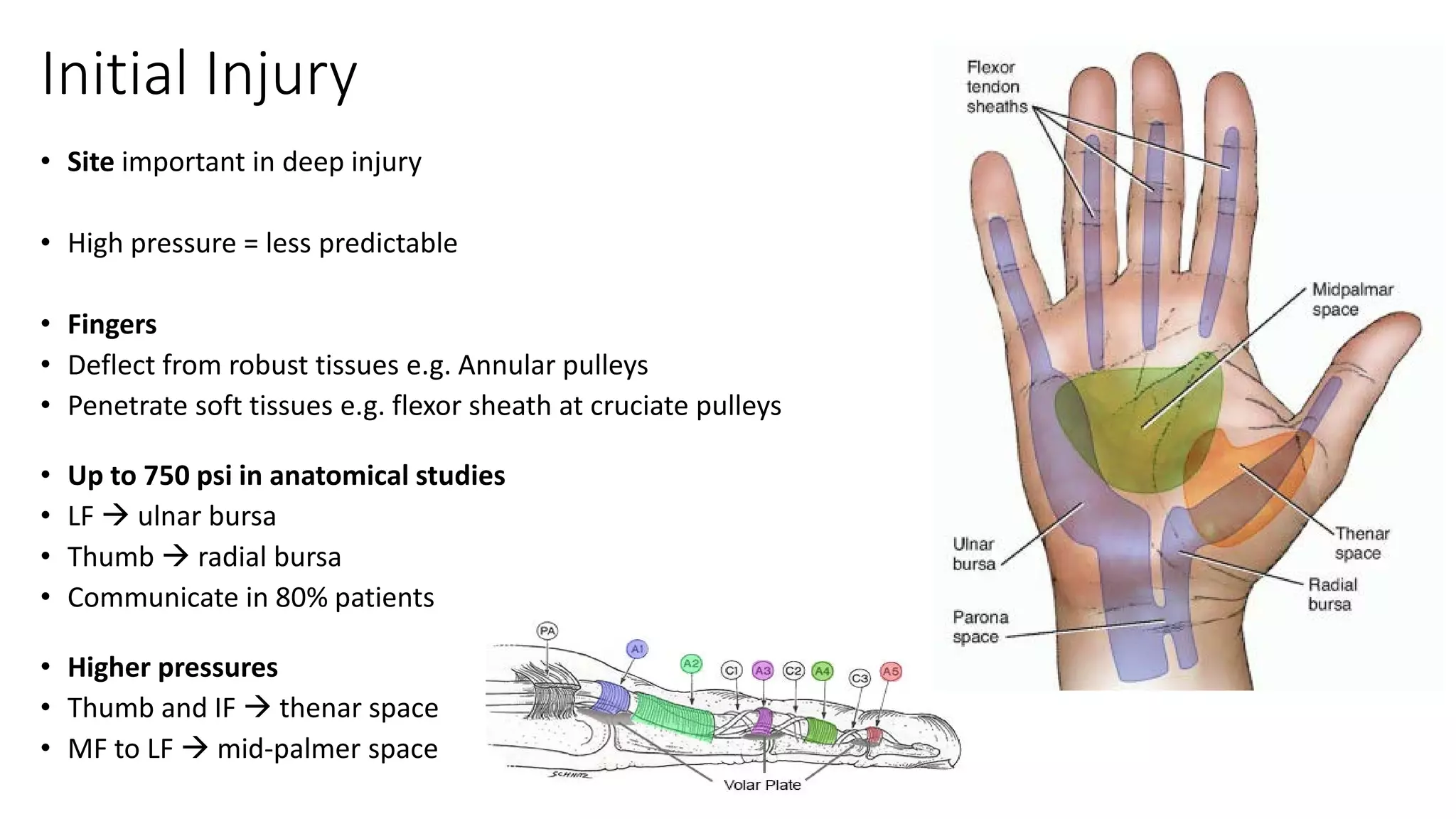


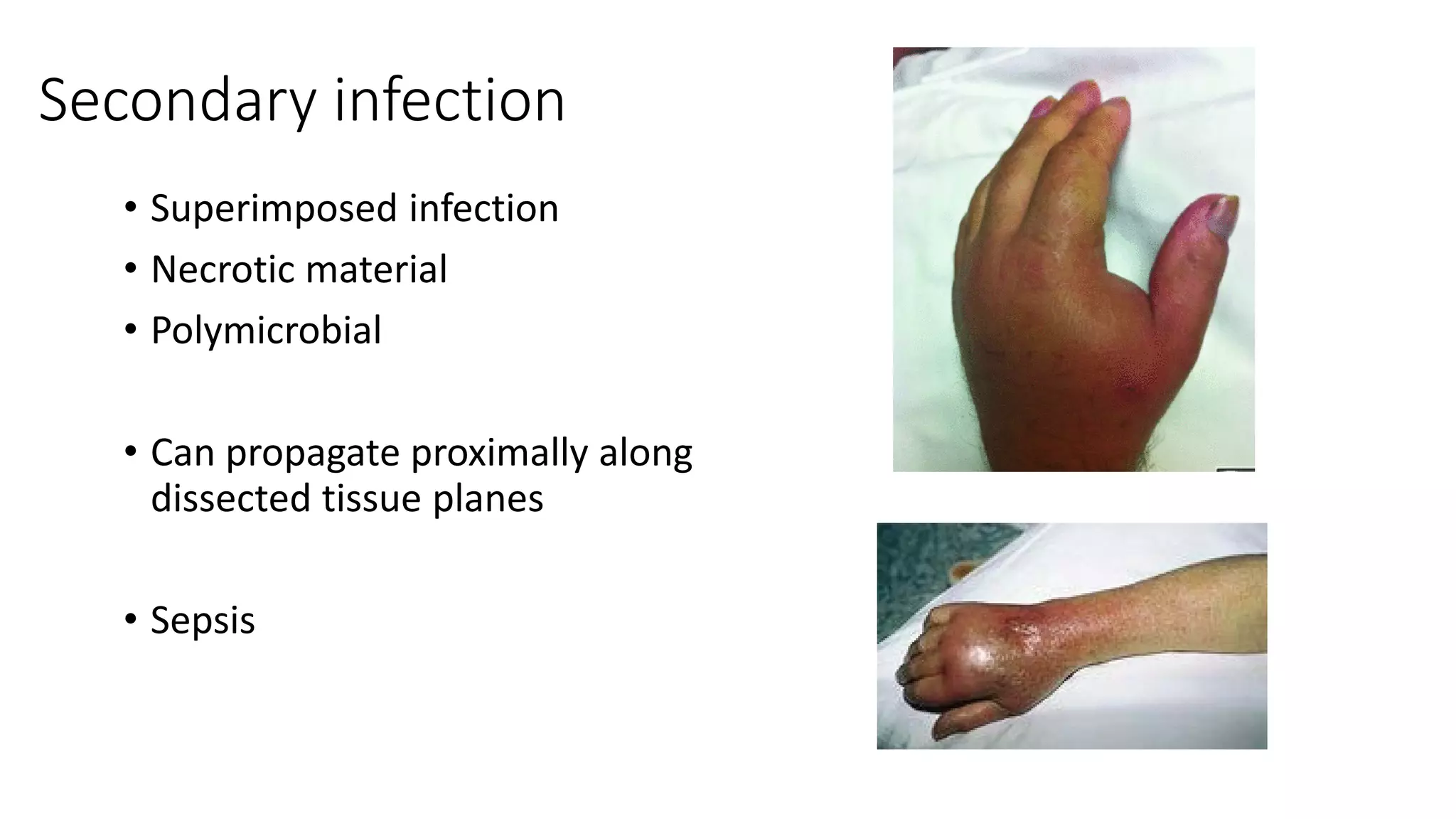



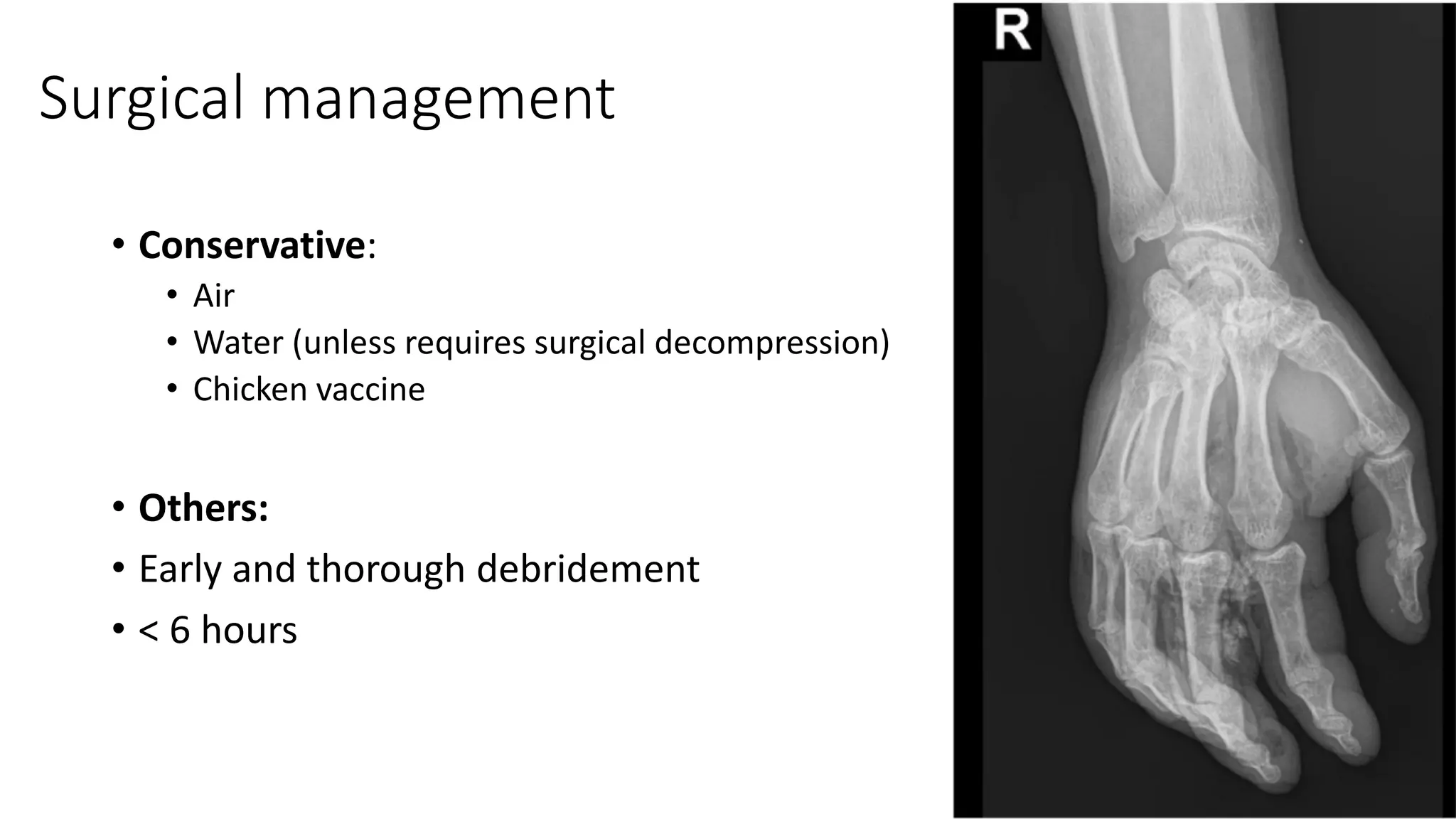
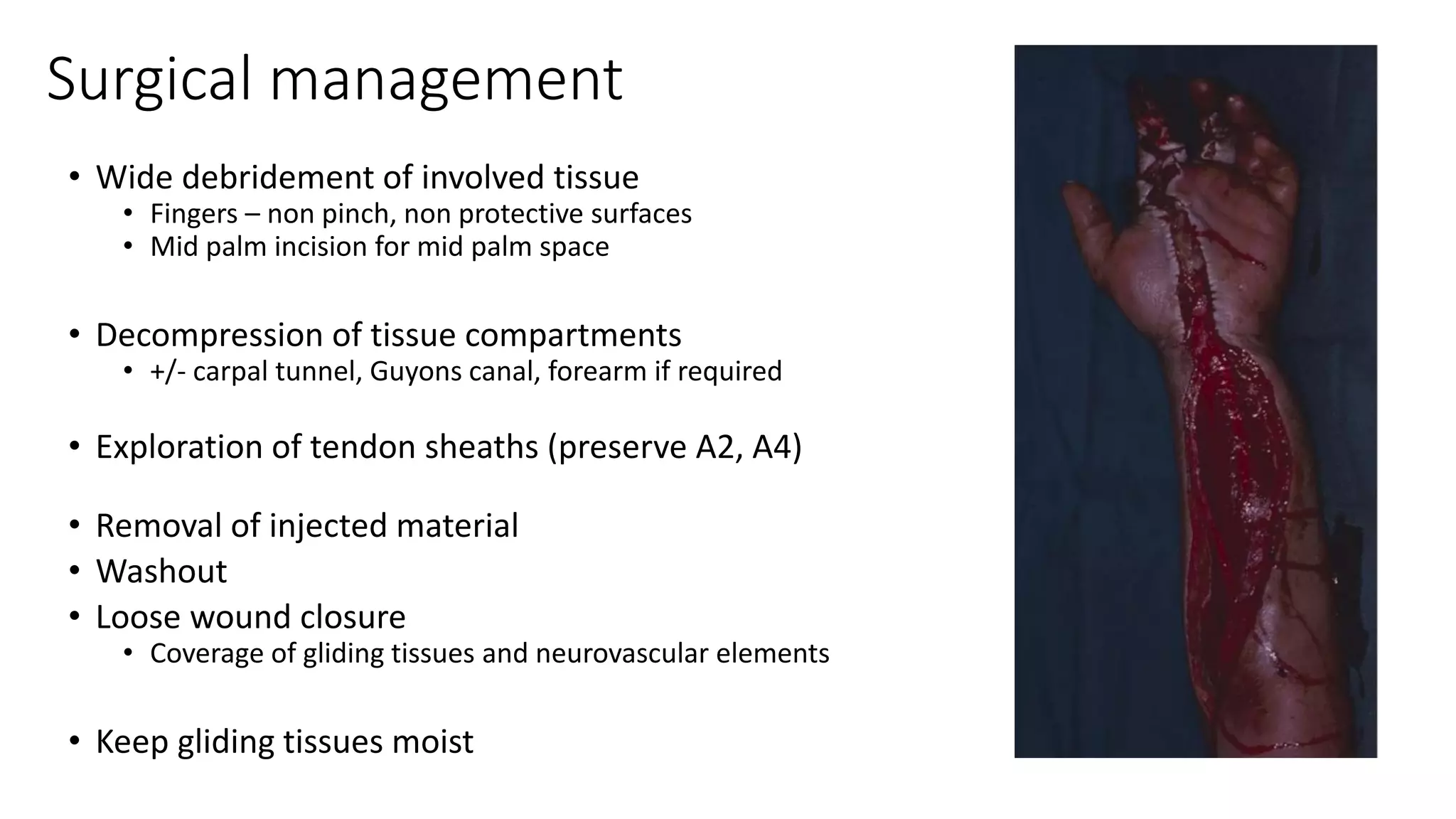

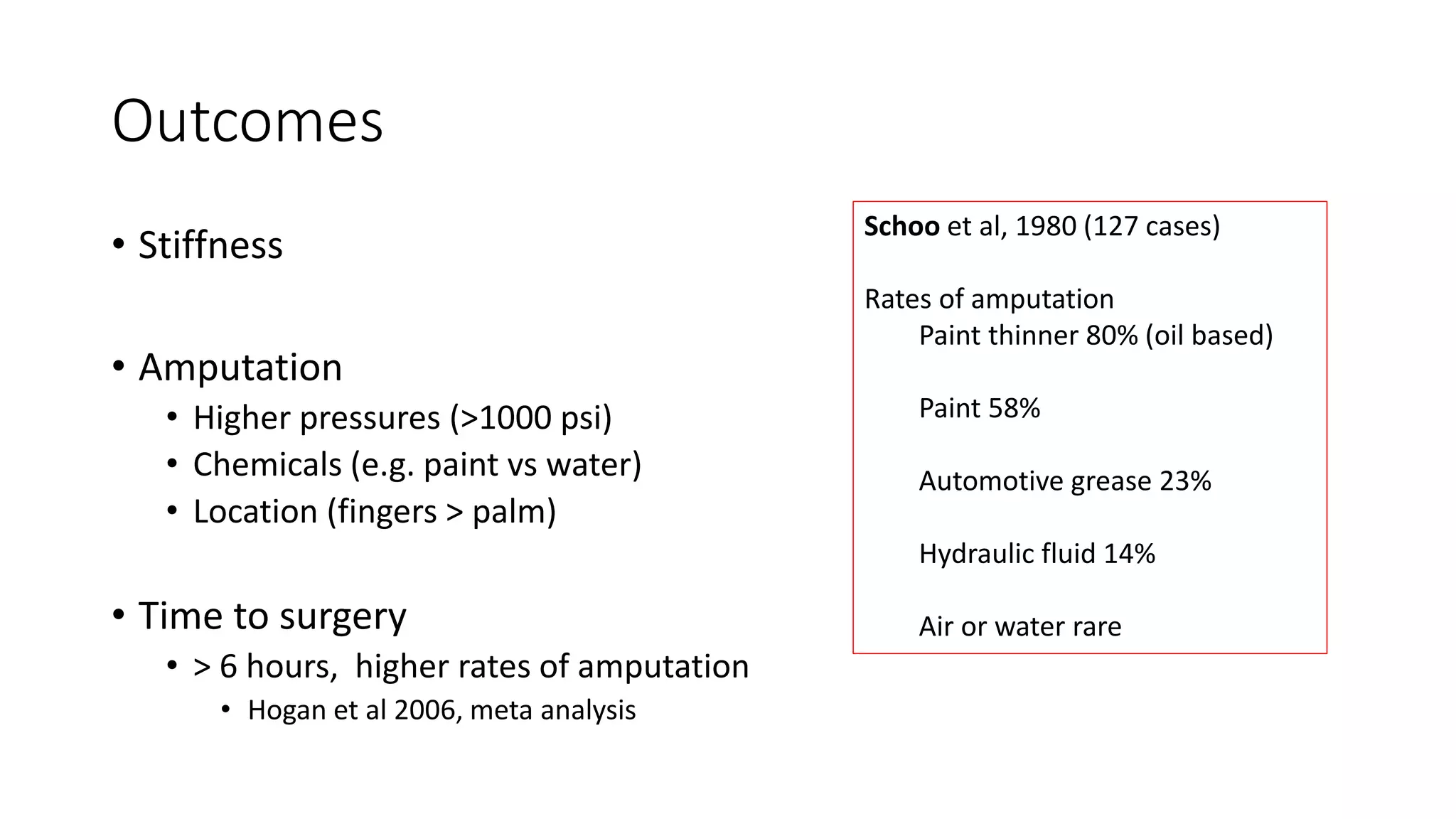




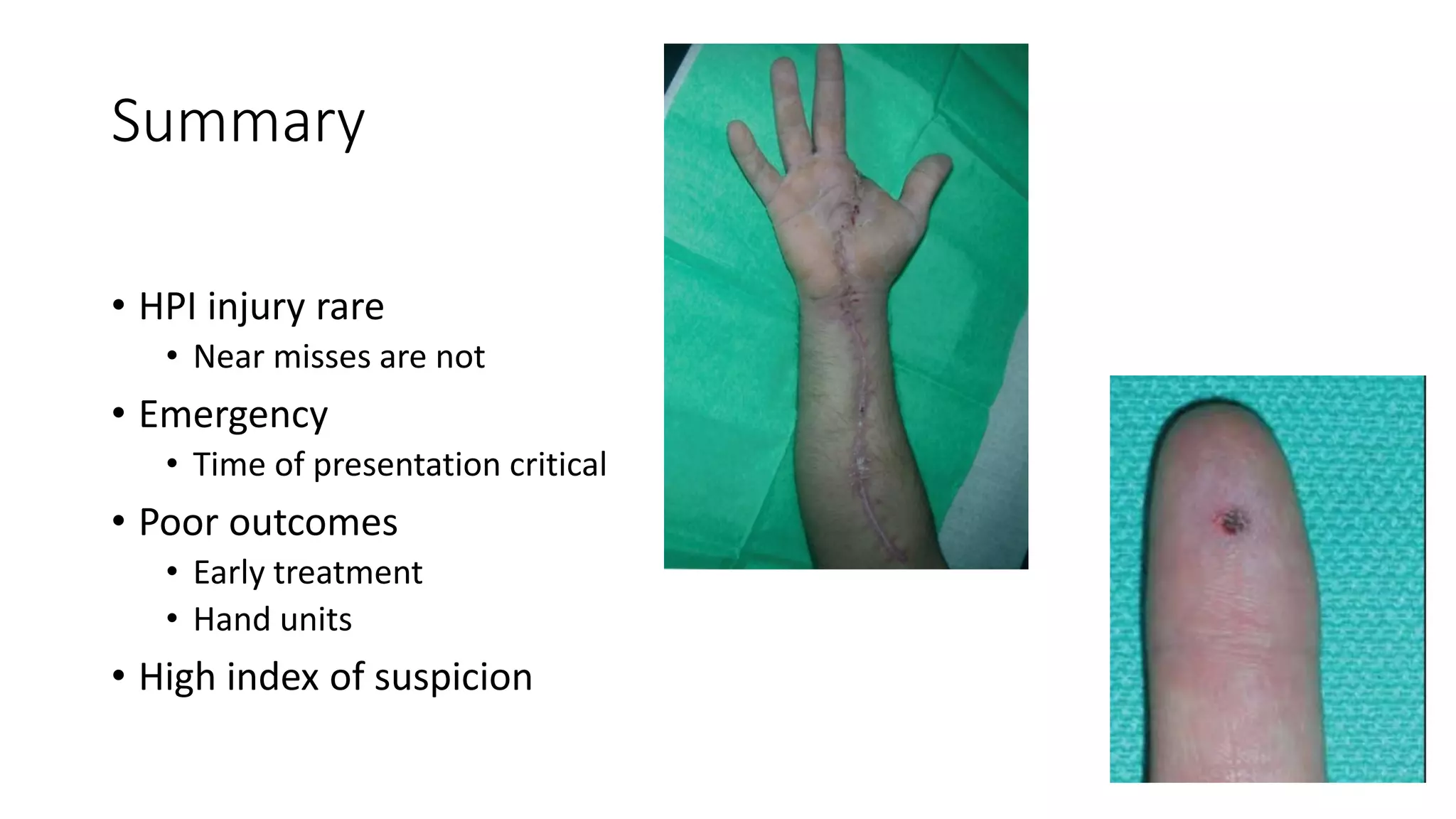


High pressure injection injuries to the hand are surgical emergencies that require timely treatment to prevent infection, necrosis, and potential amputation. While such injuries are rare occurrences, the initial injury can dissect tissue along planes of least resistance, damaging neurovascular bundles. Local chemical irritation from substances like paint or grease also induce a severe inflammatory response. Without early thorough debridement within 6 hours, the injected material and damaged tissue promote secondary infection that can spread proximally. Even with treatment, outcomes depend on several factors like the pressure and chemicals involved as well as the location, with injuries to the fingers having poorer prognoses than the palm.


















































































