1) The document discusses classification and management of wounds, principles of wound healing, haemorrhage and bleeding control. It covers types of wounds, wound assessment, classification, management, healing process, complications and haemostasis.
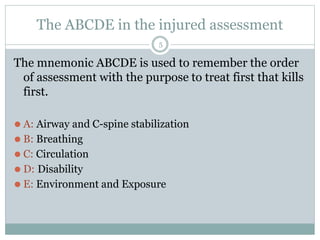
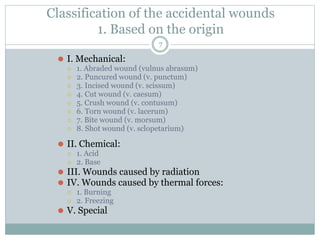
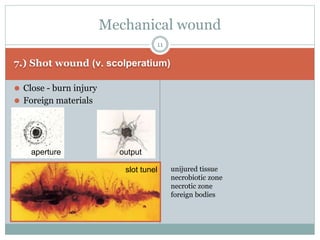
2) Wounds are classified based on origin (mechanical, chemical, thermal, radiation), depth, and bacterial contamination. The ABCDE method is used for injury assessment. Proper wound management includes cleaning, dressing, and closure techniques.
3) Wound healing involves haemostasis, inflammation, proliferation, and remodeling. Factors like infection, ischemia, and nutrition can impact healing. Complications include seromas, disruptions, and hypertrophic scarring.
4