Downloaded 18 times



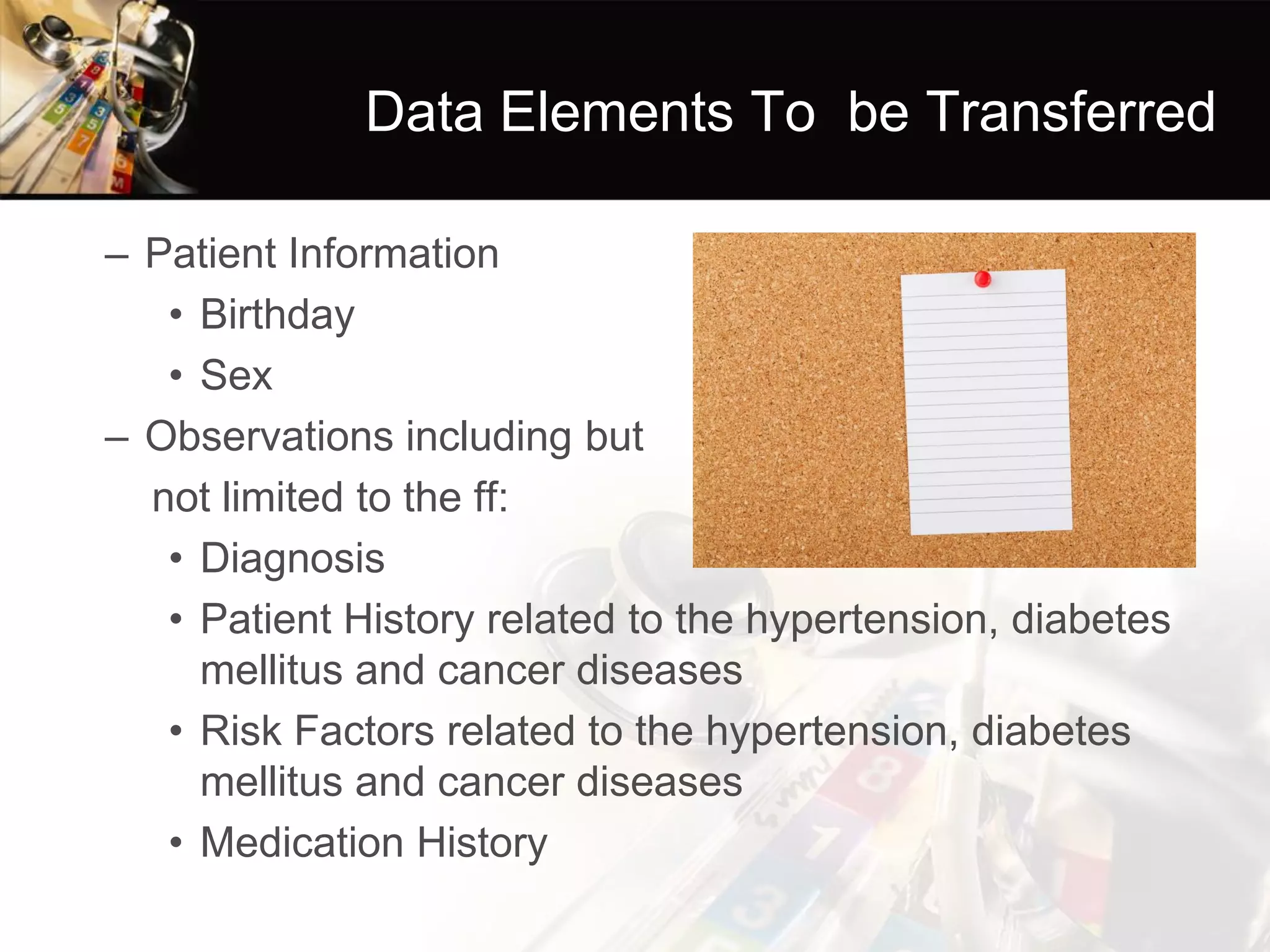
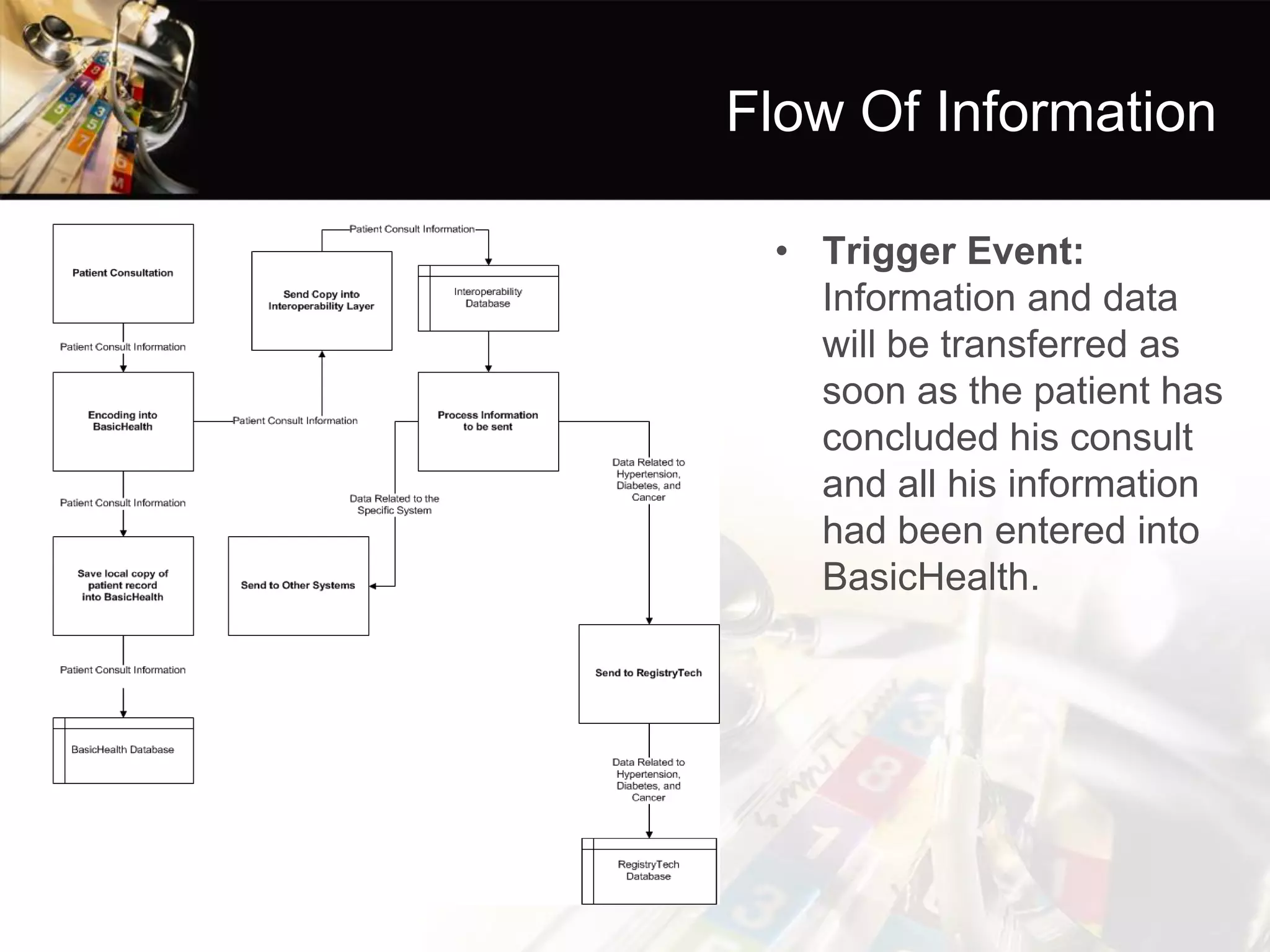

The document discusses healthcare interoperability and standards, focusing on how disparate healthcare systems can share critical patient information. It presents a specific scenario involving local health units and their use of an electronic medical record system to report cases of chronic diseases to a national registry. Key goals include improving information flow, data accuracy, and establishing standards to ensure consistency across different applications.