Downloaded 40 times

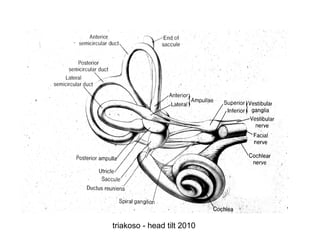


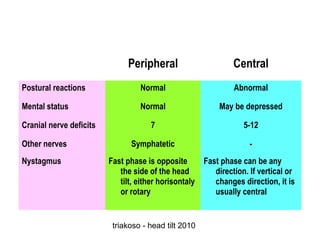


This document discusses head tilt, which is a tilting of the head away from its normal orientation associated with disorders of the vestibular system. It describes the pathophysiology of the vestibular system and how head tilt relates to lesions affecting this system. Potential causes of head tilt are discussed, including peripheral diseases such as otitis and central diseases such as tumors. Signs, diagnostic testing, treatment, and medications associated with different underlying causes of head tilt are outlined.









































































