Downloaded 44 times

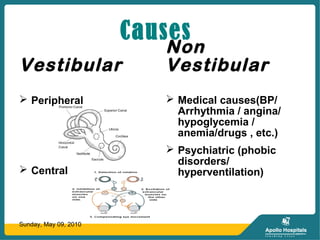
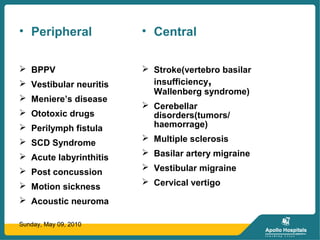
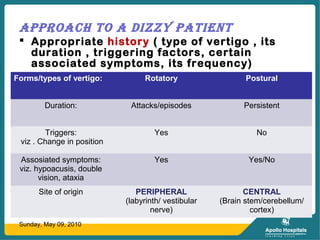


This document discusses dizziness and vertigo. It begins by defining vertigo as a spinning or whirling sensation originating from the Latin word "vertö." It then provides more definitions and describes the different causes of vertigo including peripheral and central vestibular causes, medical causes, and psychiatric causes. The document outlines the approach to evaluating a dizzy patient and describes various vestibular tests. It discusses management options for vestibular disorders including physiotherapy, medical management, psychological therapy, and surgery. Specific conditions like BPPV, Meniere's disease, and vestibular neuritis are also described.































![Vertigo Usa Presentation Auto Scott[1]](https://cdn.slidesharecdn.com/ss_thumbnails/vertigousapresentationautoscott1-124717933195-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)






















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
