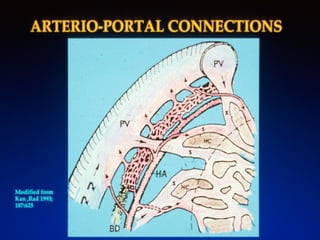
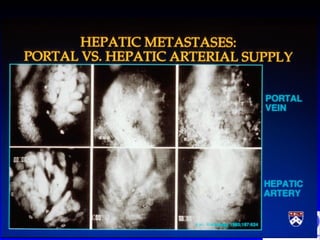
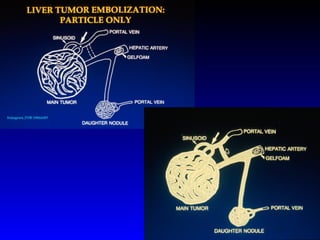
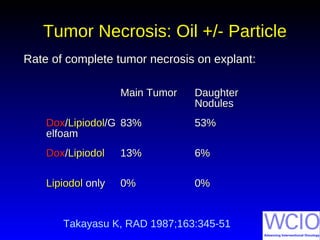
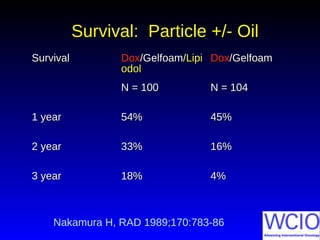
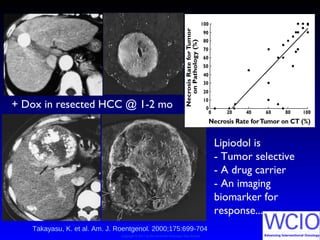
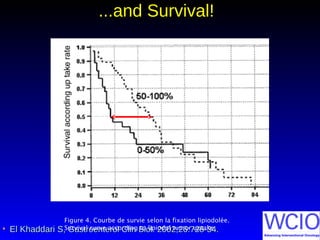
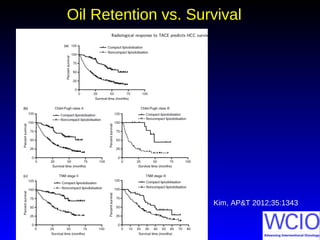
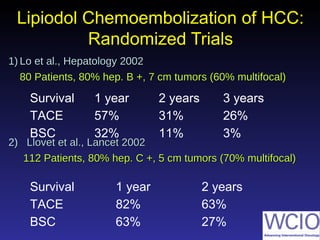
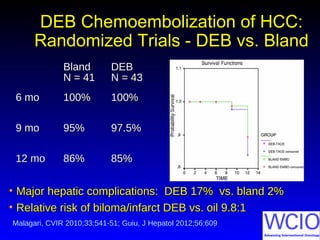
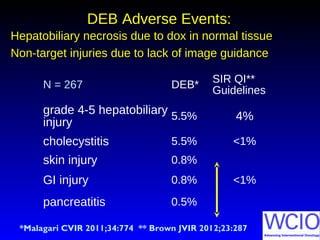
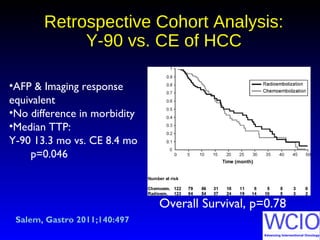
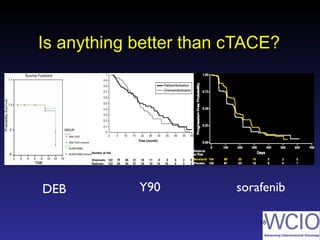
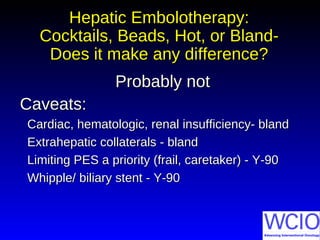
This document discusses various methods of embolization for hepatocellular carcinoma (HCC), including the use of cocktails, beads, radioactive spheres, and bland embolization. It provides a brief history of the use of Lipiodol as a drug carrier and imaging biomarker. Randomized trials are summarized that compare chemoembolization using doxorubicin-eluting beads or Lipiodol to bland embolization or best supportive care, showing improved survival with the addition of chemotherapy. Adverse events are higher with doxorubicin-eluting beads compared to Lipiodol or bland embolization due to increased risk of hepatobiliary necrosis and non-target embolization.

![15
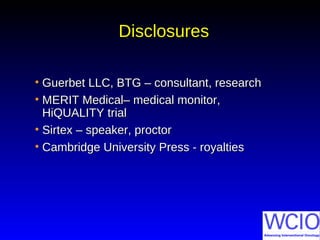
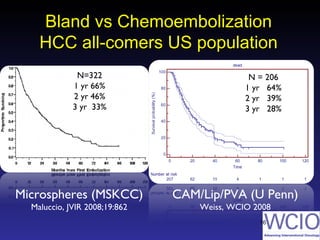
What about bland?What about bland?
15
1-year 2-year 3-year HR
Control 63% 27% 17%
Chembo 82% 63% 29% 0.47 [0.25-0.91]
p=0.02
Bland 75% 50% 29% 0.57 [0.31-1.04]
p=0.07
Llovet, Lancet 2002](https://image.slidesharecdn.com/10301100-michael-soulen-pairs-2014-hcc-embo-2-160212103050/85/HCC-EMBOLIZATION-21-320.jpg)



















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








