Downloaded 192 times
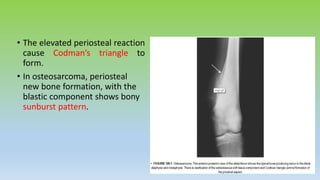

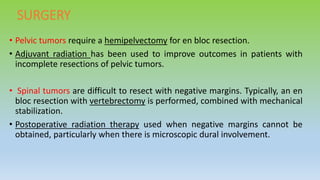

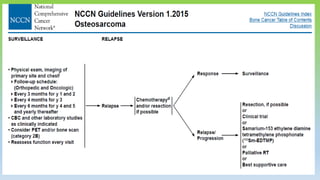


Osteosarcoma is the most common primary bone cancer, often arising in the appendicular skeleton of teenagers and young adults. It is typically a high grade tumor associated with rapid bone proliferation and spread. Treatment involves complete surgical resection with limb-sparing surgery when possible, along with chemotherapy both before and after surgery. Radiation therapy may be used for unresectable or incompletely resected tumors. Prognostic factors include tumor size, location of metastases, and response to preoperative chemotherapy. While survival has improved with modern multimodal treatment, new strategies are still needed given the risk of recurrence and lung metastases.



































































