Download to read offline
![Retained HTXs…
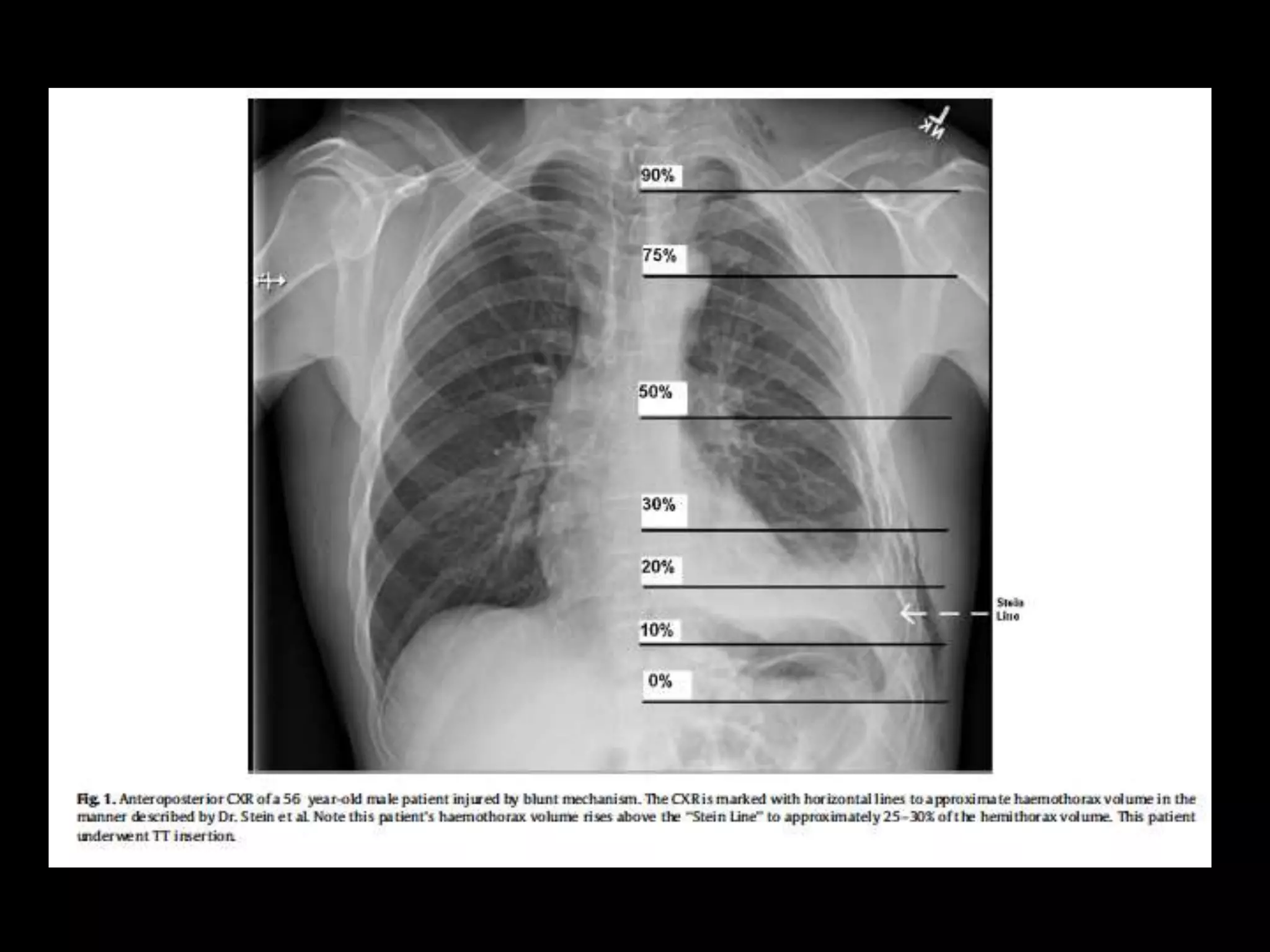
“…I need to know an answer to a different question…and that is,
of a given size hemothorax without intervention what is the
likelihood of that leading to… [complications]”
Dr. J. Wayne Meredith (Winston-Salem, NC)
J Trauma. 2011;72(1):11-24](https://image.slidesharecdn.com/ql1o5ajzsea5au0mzvf2-signature-c3892c1531cffad395203f49f323b2f61492a567c70fd70f6b8ce24eeb47f099-poli-190814044238/75/Haemothorax-To-drain-or-not-to-drain-8-2048.jpg)
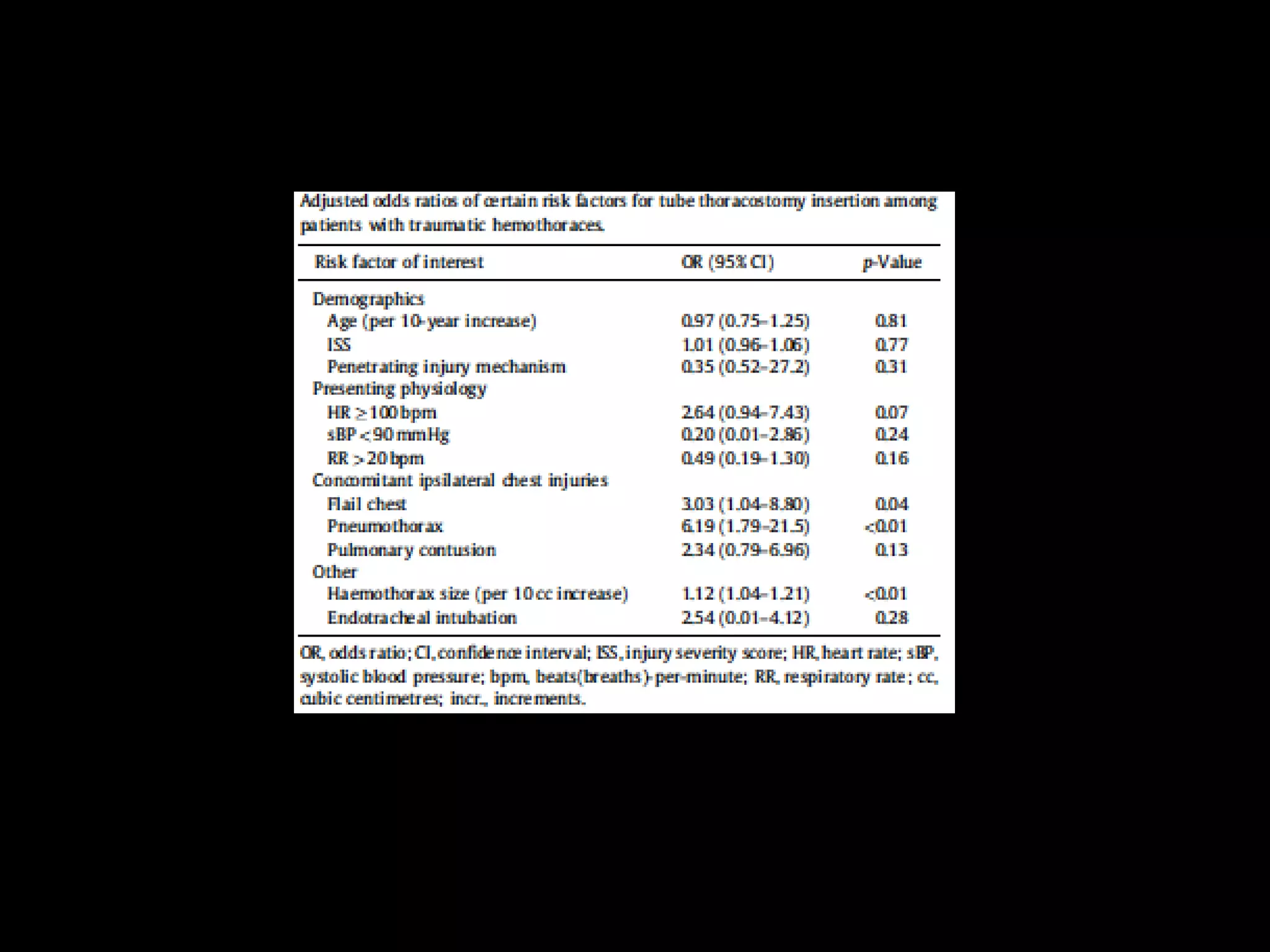
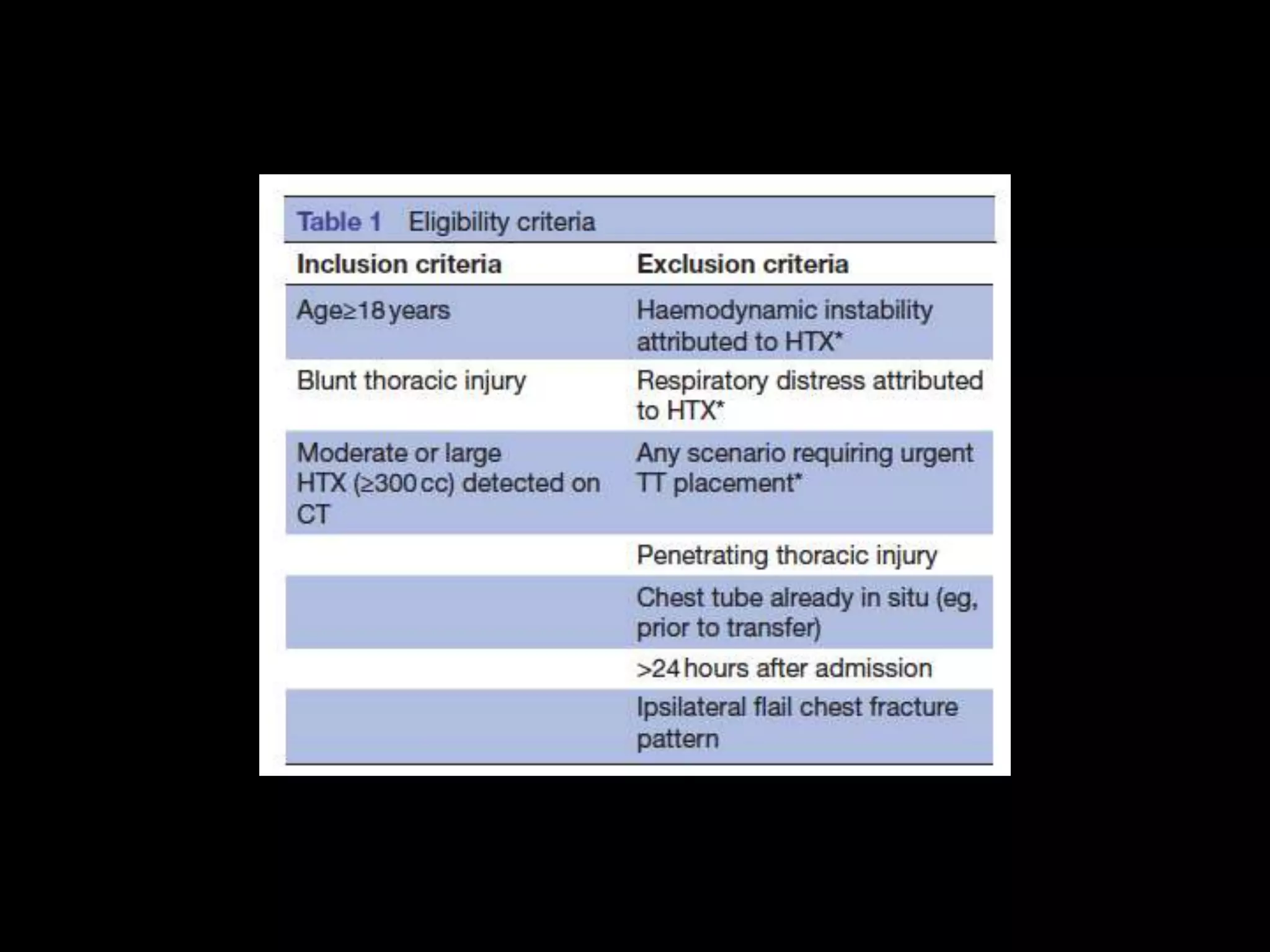
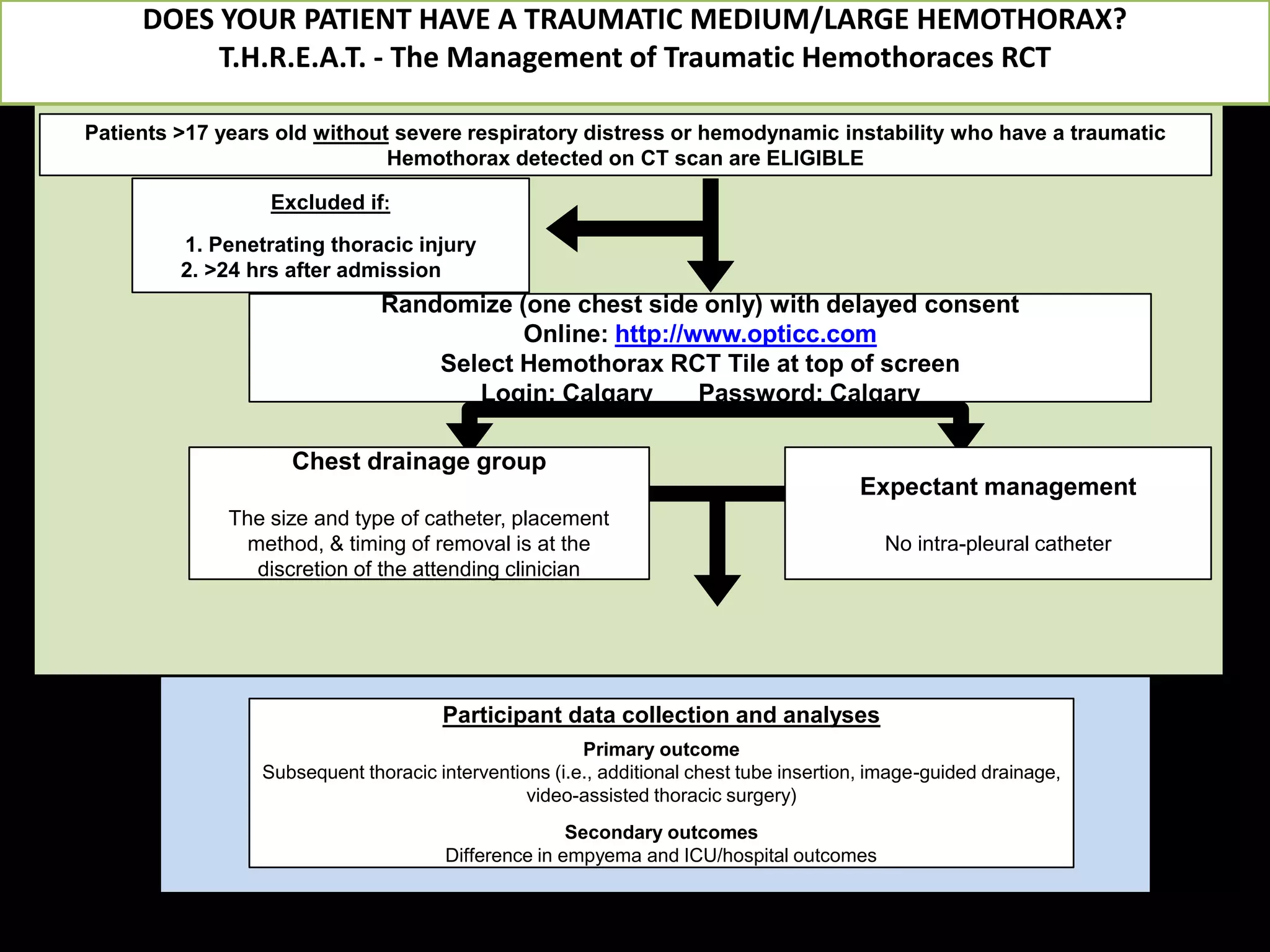


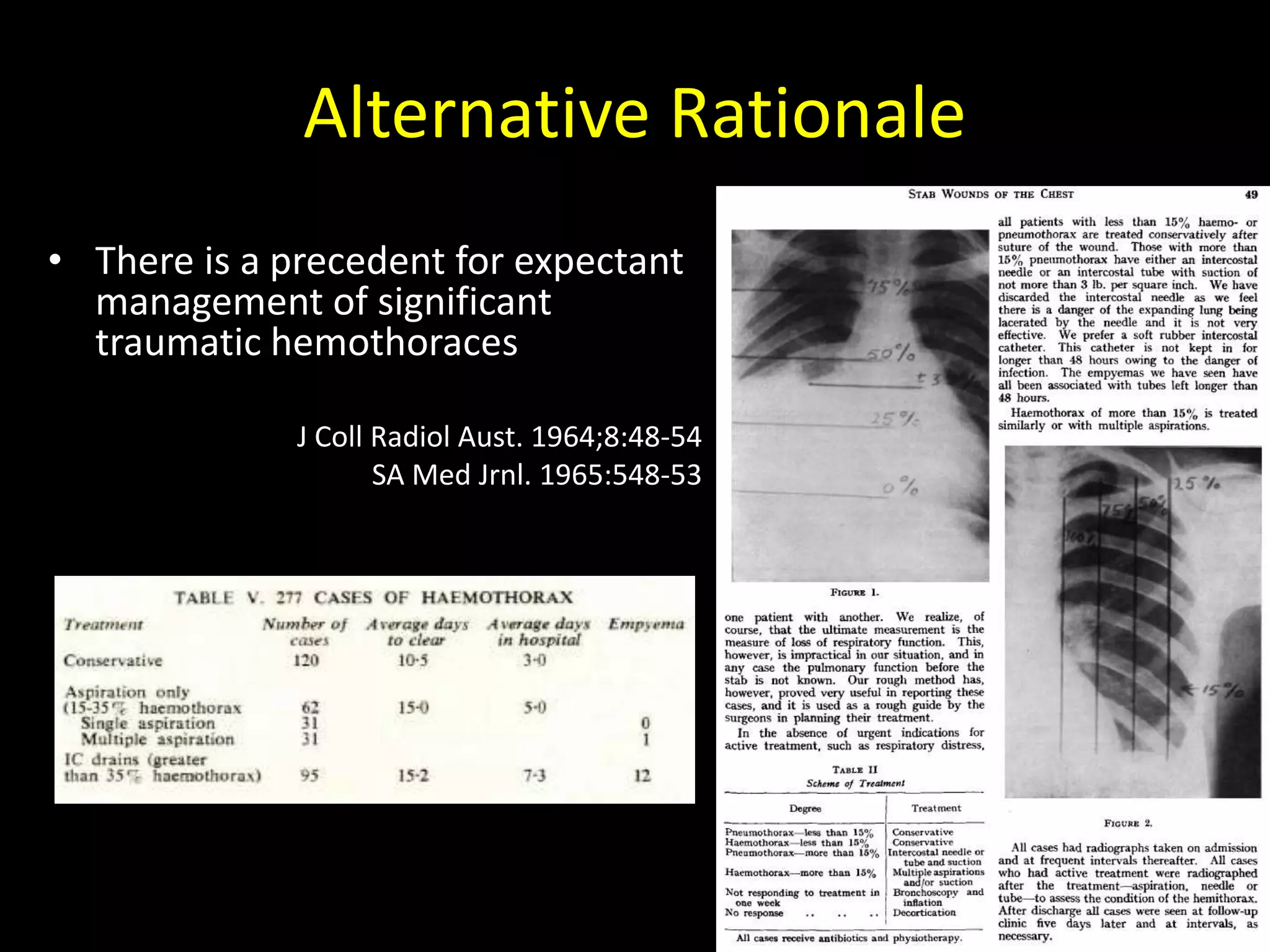
1) The document discusses whether all traumatic hemothoraces should undergo drainage or if some can be managed expectantly. 2) Recent studies have found that expectant management of hemothoraces may have benefits over drainage such as shorter hospital stays and fewer complications, but larger studies are still needed. 3) The T.H.R.E.A.T. trial aims to further study this question by randomly assigning traumatic hemothorax patients either to chest drainage or expectant management and comparing outcomes between the groups.




































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)

















