Download to read offline











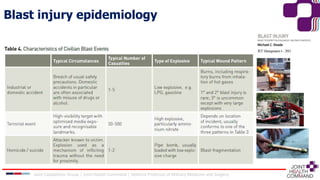



1) A bomb attack in Brussels in 2016 killed 32 people and injured 300 through the use of acetone/peroxide explosive devices in the airport and a train station. 2) Blast injuries are classified as primary (caused directly by the blast wave), secondary (caused by flying debris and shrapnel), tertiary (caused by victim being thrown by the blast), or quaternary (all other injuries). 3) While myths exist about blast injuries overwhelming hospitals and causing many amputations, in reality penetrating injuries from flying debris are most common in survivors and usually do not require extensive surgery. Management follows conventional trauma principles.














































































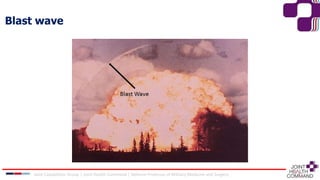
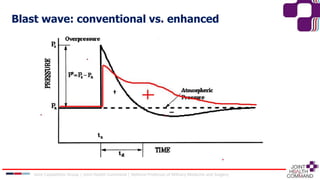
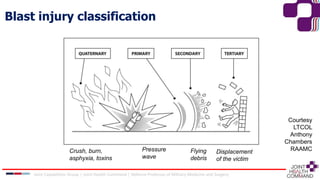
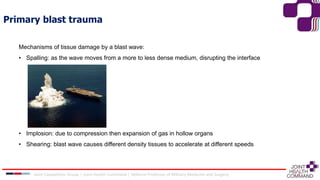
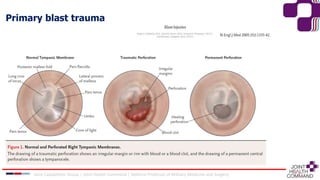
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







