Downloaded 20 times


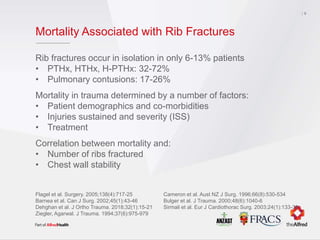


Rib fractures are common injuries that can have significant morbidity and mortality. While several randomized controlled trials have shown benefits of surgical stabilization for flail chest injuries, national guidelines conditionally recommend rib fixation only for flail injuries. Recent large observational studies suggest mortality may be lower with surgery for flail chest. Further research is still needed to determine if surgical stabilization provides benefits for non-flail rib fractures.





![Air leaks in Thoracic Surgery [Auto-saved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/airleaksinthoracicsurgeryauto-saved-230219163120-6180857a-thumbnail.jpg?width=640&height=640&fit=bounds)

















































































