Download to read offline

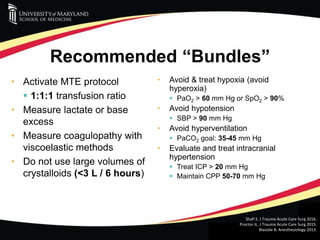
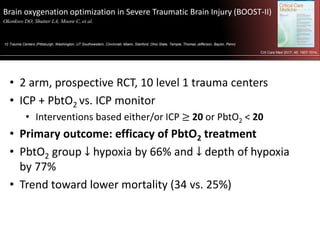
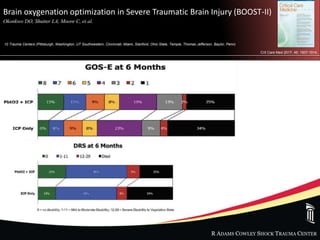
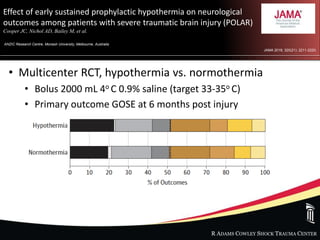
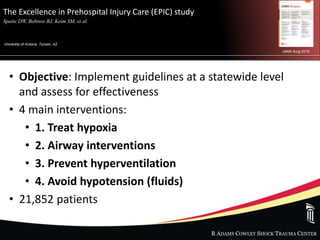
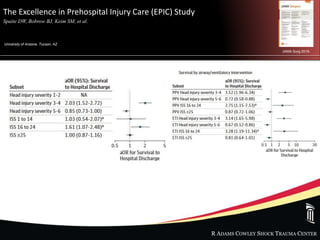


This document summarizes recent literature on the treatment of traumatic brain injury (TBI). It reviews guidelines for managing TBI, including avoiding hypotension and hypoxia. It discusses studies on fluid resuscitation with hypertonic saline or plasma. The document also summarizes three important TBI studies: the BOOST-II trial on brain oxygen monitoring, the POLAR trial on early hypothermia, and the EPIC statewide study implementing prehospital TBI guidelines. Throughout, it notes limitations of animal studies in reproducing complex human TBI pathophysiology and outcomes.











































![Traumatic brain injury [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/traumaticbraininjuryautosaved-230313134042-a66a1551-thumbnail.jpg?width=640&height=640&fit=bounds)























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















