


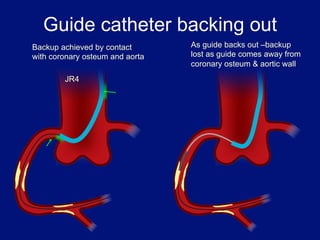
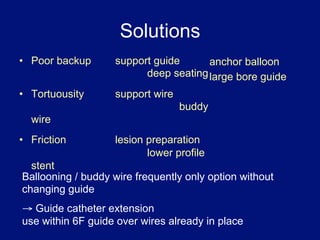
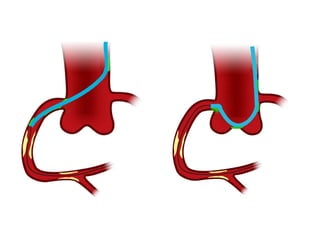
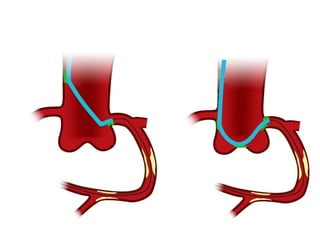
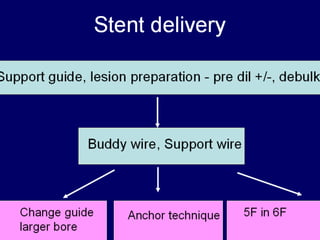
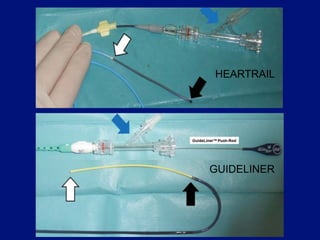
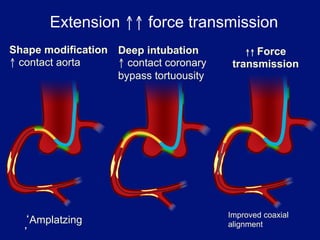
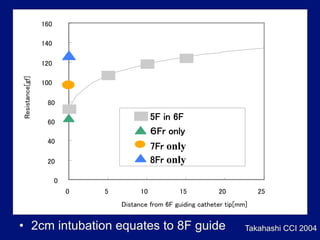
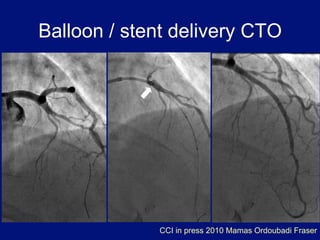
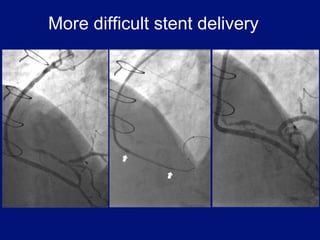
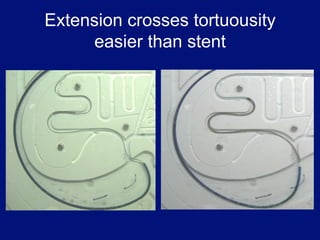

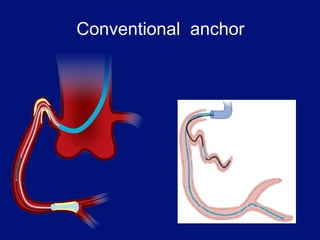
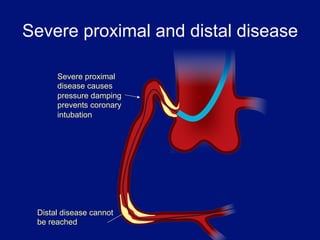
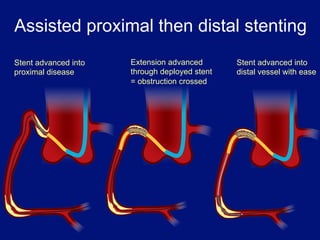
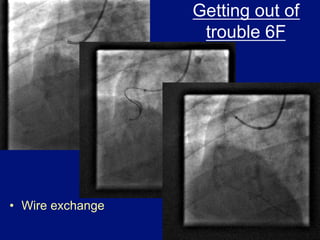
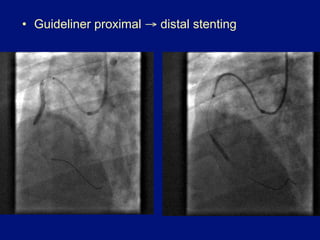
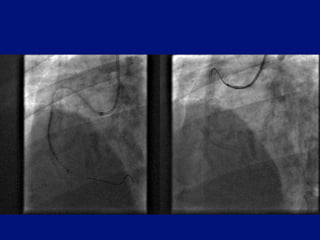
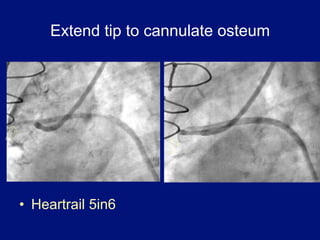
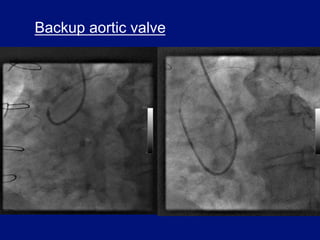
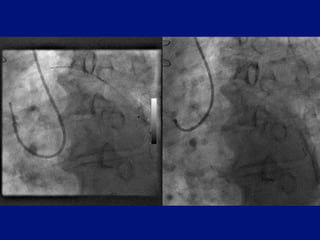
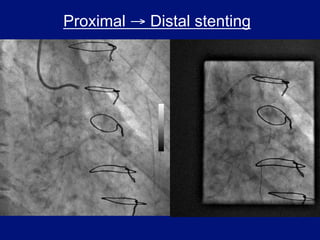
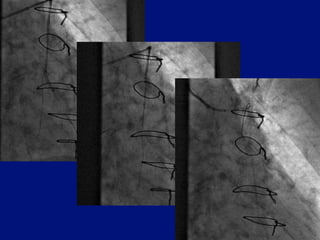
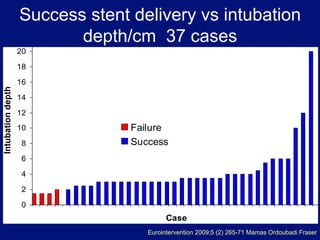
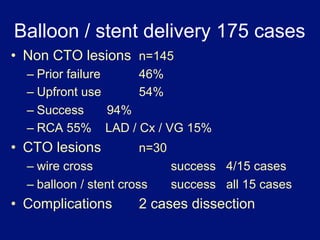
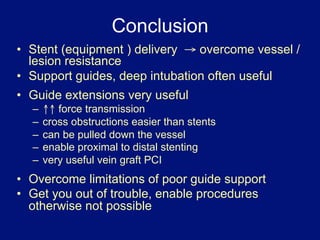
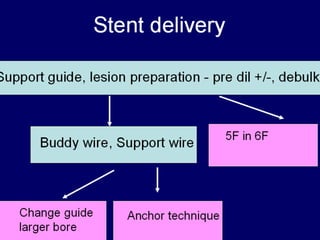
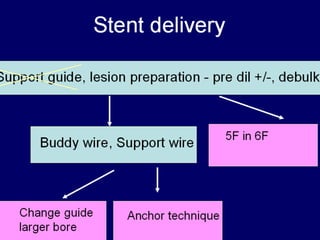
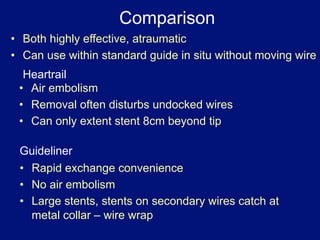
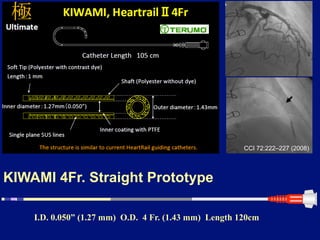
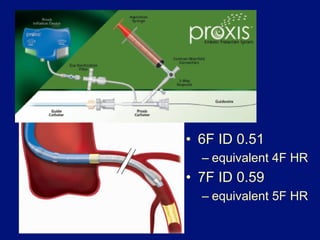
This document discusses methods for optimizing backup support when performing percutaneous coronary interventions (PCIs). It describes how guide catheters can lose backup support as they are withdrawn from the coronary ostium and aorta. Solutions proposed include using anchor balloons, buddy wires, and lesion preparation to improve friction. Guide catheter extensions are highlighted as an effective way to increase backup support, enable deeper seating, improve force transmission, and allow proximal-to-distal stenting by bypassing tortuous vessels or deployed stents. Data is presented showing high success rates for stent delivery with extensions. In conclusion, guide extensions are a useful tool for overcoming vessel resistance and limitations of poor guide support to enable procedures that may otherwise not be possible












































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









