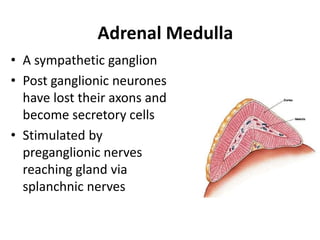
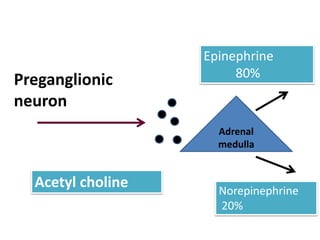
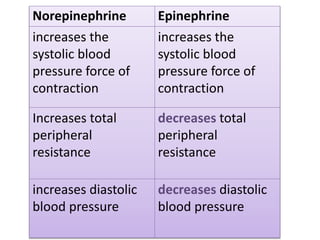
The document discusses catecholamines such as epinephrine, norepinephrine, and dopamine that are produced in the adrenal medulla in response to stress. These catecholamines act on alpha and beta adrenergic receptors to prepare the body for emergency situations by increasing metabolic rate, heart rate, and blood pressure through various cardiovascular and metabolic effects. The adrenal medulla is innervated by preganglionic nerves and stimulated to secrete catecholamines. Glucocorticoids are necessary for normal development of the adrenal medulla. Catecholamines are metabolized to vanillylmandelic acid which is excreted in urine. Pheochromocytoma is a tumor