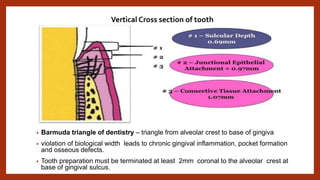
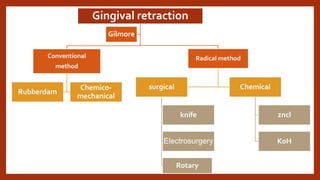
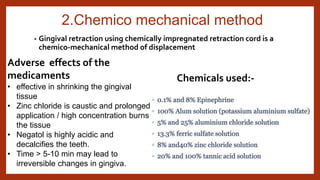
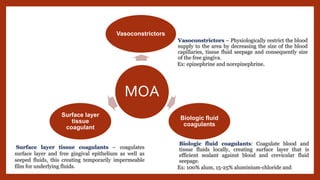
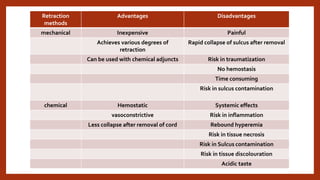
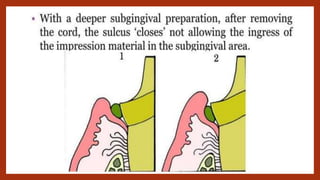
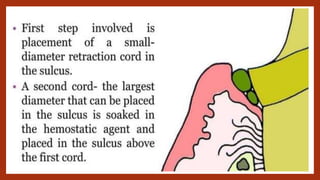
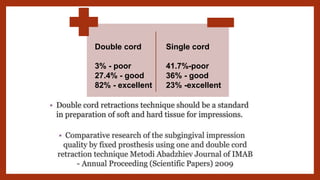
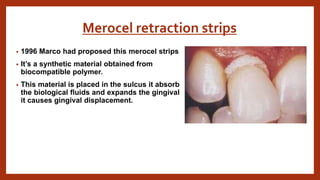
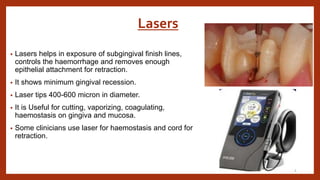
This document discusses various methods for gingival retraction to expose the tooth structure beneath the gingiva. It describes mechanical, chemico-mechanical, and surgical retraction methods. Mechanical methods include use of retraction cords, while chemico-mechanical methods involve chemically-treated cords to shrink gingival tissue. Recent advances discussed include laser retraction and cordless techniques like Expasyl paste that cause less trauma than cords. Proper technique and material selection are important to effectively retract tissue without damaging the periodontium.















































































![anatomical landmarks [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/anatomicallandmarksautosaved-231230051158-4ead7005-thumbnail.jpg?width=640&height=640&fit=bounds)




















