Madan Bhandari Academyof Health Sciences
Renal Function Tests
Presented by:
Laxman Pariyar
2nd
batch/6th
sem
MBAHS
2.
Madan Bhandari Academyof Health Sciences
Overview:
• Introduction
• Laboratory tests
– Biochemical tests of Renal function
– Urinalysis
– Measurement of Glomerular function
– Tubular function test
• Renal Failure
– Acute Renal Failure
– Chronic Renal Failure
– Renal Tubular Disorders
3.
Madan Bhandari Academyof Health Sciences
Introduction
- Major functions of the kidneys:
• Excretion of metabolic waste products
• Maintenance of water, pH, and electrolyte balance
• Production of calcitriol and erythropoietin
• Decrease in kidney function linked to reduced performance of nephrons
• Functional unit of the kidney is nephron
4.
Madan Bhandari Academyof Health Sciences
Components of the nephron
• Bowman’s capsule with glomerular tuft of capillaries
• Proximal convoluted tubule (PCT)
• Loop of Henle
• Distal convoluted tubule (DCT)
• Collecting tubules
5.
Madan Bhandari Academyof Health Sciences
Laboratory tests
• Classification of renal function tests
I. To screen for kidney disease
– Biochemical tests of Renal function
Plasma urea and creatinine
Plasma electrolytes
– Complete urine analysis
6.
Madan Bhandari Academyof Health Sciences
Conti…
II. To assess renal function:
a. To assess glomerular function
Glomerular filtration rate
Clearance tests
Glomerular permeability
Proteinuria
b. To assess tubular function
Reabsorption studies
Secretion tests
Concentration and dilution tests
7.
Madan Bhandari Academyof Health Sciences
To screen for kidney disease
• Biochemical tests of Renal function
– Urea
o Urea is freely filtered by the glomerulus.
o Approximately 40% of urea is actively reabsorbed by the tubules.
o Rate of urea reabsorption varies inversely with tubular flow.
o Urea concentration in urine is about 70 times higher than in plasma.
o Urea constitutes 80% of total urinary solutes.
o Urine is approximately a 2% solution of urea.
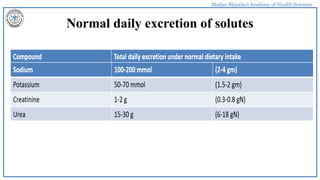
o The reference interval for serum urea of healthy adults is 10-40 mg/dl. Urinary excretion of
urea is 15 to 30 g/day
8.
Madan Bhandari Academyof Health Sciences
Conti…
Non-renal factors can affect the urea level (normal adults is level 10-40mg/dl)
like:
• Mild dehydration,
• high protein diet,
• increased protein catabolism, muscle wasting as in starvation,
• reabsorption of blood proteins after a GIT haemorrhage
9.
Madan Bhandari Academyof Health Sciences
Conti…
States associated with elevated levels of urea in blood are referred to as uremia or
azotaemia.
Causes of urea plasma elevations:
• Pre-renal: renal hypoperfusion
• Renal: acute tubular necrosis
• Post-renal: obstruction of urinary flow
10.
Madan Bhandari Academyof Health Sciences
Increased serum creatinine:
– Impaired renal function
– Very high protein diet
– Anabolic steroid users
– Vary large muscle mass: body
builders, giants, acromegaly patients
– crush injury
– Athletes taking oral creatinine.
Madan Bhandari Academyof Health Sciences
Creatinine
– Creatinine is neither reabsorbed nor secreted.
– The urinary concentration is about 70% that of plasma.
– Considered as a surrogate marker of GFR
– Late indicator of kidney dysfunction
– Normal range is 0.8-1.3 mg/dl in men and 0.6-1 mg/dl in women. Urinary
excretion 1-2gm/day
13.
Madan Bhandari Academyof Health Sciences
• Sodium
– absorption from proximal convoluted tubules by co-transport mechanism
involving sodium, glucose, and amino acids
– Coupled with sodium-potassium-ATPase activity
• Potassium
– approximately 70% of potassium is reabsorbed by proximal convoluted tubules
– net secretion of K+ occurs at distal tubules
Madan Bhandari Academyof Health Sciences
Complete urine analysis
Complete urine analysis includes physical examination of urine,
chemical examination (to find out the abnormal constituents
present in the sample) and microscopic examination
Urine sample may be: 24 hours urine (preferred) or spot urine
(mid stream clean catch)
Madan Bhandari Academyof Health Sciences
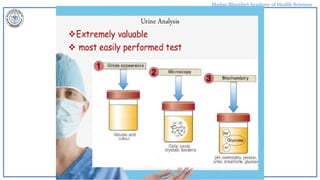
Urine Analysis
It includes, physical examination
• Volume: 800-2500 ml/day. It depends on water intake, temperature, diet, CVS
& renal disorder
• Polyuria: >2500 ml/day. DM, DI, chronic Glomerulonephritis
• Oligouria: Up to 500 ml/day. Fever, diarrhea, nephritis, glomerulonephritis,
cardiac failure.
• Anuria: <50 ml/day. Renal failure, Renal failure
18.
Madan Bhandari Academyof Health Sciences
Appearance
• Normal urine is transparent pale yellow colour. Variation in colour may
be physiological or pathological.
• Reddish colour- Stones, injury, Diseases in kidney.
• Darkening- presence of pigment. i.e. haemoglobin & myoglobin in urine.
• Turbidity may indicate the UTI.
19.
Madan Bhandari Academyof Health Sciences
Conti…
• PH- Determinations of urinary PH- fresh sample.
• Acidic in reaction, Normal PH Range 5.5-7.5.
• Acidic PH- acidosis and high protein diet.
• Alkaline PH- low protein diet
20.
Madan Bhandari Academyof Health Sciences
Conti…
• Specific gravity: It is varies from 1.005-1.025
It is depend on the concentration of dissolved total solids.
• Sp. gravity can vary in pathological cases:
low- 1.001-1.003 in DI,, Glomerulonephritis.
• High- in DM, congestive heart failure, dehydration
• Fixed SG is 1.010 is seen in severe Renal damage, Anuria.
21.
Madan Bhandari Academyof Health Sciences
Chemical examination:
• It includes detection of the following Glucose, protein, blood.
Glucose: *Excretion of detectable amount of reducing
sugar in urine is called as Glycosuria.
Protein: Increased amount of protein in urine called
as proteinuria.
Causes: ed Glomerular Permeability
tubular reabsorption.
• Blood: Presence of blood in urine is called as Haematuria.
• Causes: Injury, diseases of kidney, UTI, renal stones, cancer.
22.
Madan Bhandari Academyof Health Sciences
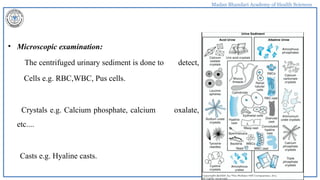
• Microscopic examination:
The centrifuged urinary sediment is done to detect,
Cells e.g. RBC,WBC, Pus cells.
Crystals e.g. Calcium phosphate, calcium oxalate,
etc....
Casts e.g. Hyaline casts.
23.
Madan Bhandari Academyof Health Sciences
Measurement of Glomerular function
• Inulin clearance
• Creatinine clearance
• Plasma Creatinine
• Calculated creatinine clearance
• Estimated GFR
• Cystatin C
• Plasma urea concentration
• Plasma β2-microglobulin
• Isotopic technique for measuring GFR
24.
Madan Bhandari Academyof Health Sciences
TESTS FOR GLOMERULAR FUNCTION:
GFR:
The total quantity of filtrate formed in all the nephrons of both the kidneys
in the given unit time is called as GFR.
Normal values: 125ml /min. &
about 180 lit/ day.
25.
Madan Bhandari Academyof Health Sciences
Renal clearance test
• The volume of blood or plasma completely cleared of a substance per unit time.
Expressed in millilitre of plasma per minute.
• In other word clearance of substance refers to the millilitres of plasma which
contains the amount of that substance excreted by kidney per minute.
• This can easily be calculated by measuring the clearance of plasma compound which
is freely filtered by glomerulus and is neither absorbed nor secreted in the tubule.
• The two compounds namely creatinine and urea are commonly employed for this
purpose.
26.
Madan Bhandari Academyof Health Sciences
Conti…
Clearance = U × V
P
• U- Conc. Of substance in urine
• P- Conc. Of the substance in plasma or serum
• V- the ml of urine excreted per minute. Value expressed in ml/min.
27.
Madan Bhandari Academyof Health Sciences
Creatinine clearance test
• Ref. value- Male- 0.7-1.4 mg/dl.
Female- 0.6- 1.3 mg/dl.
• Creatinine is a waste product, formed from creatine phosphate.
• It is freely filtered at the glomerulus, & not reabsorbed by the tubules.
• It can be estimated by Jaffe’s reaction.
• Volume of plasma that would completely cleared of creatinine per minute
28.
Madan Bhandari Academyof Health Sciences
Procedure:
• Give 500ml of water, to a patient to promote good urine flow.
• After about 30 min.
• Ask to empty the bladder & discard the urine, exactly after 60 min.
• Again void the bladder & collect the urine & note the volume.
• Take one blood sample.
• Then calculate the values.
CC = U × V U-Conc. Urine creatinine,
P P- Conc. Plasma creatinine
V-urine flow in ml/min.
29.
Madan Bhandari Academyof Health Sciences
Conti…
• Normal range for creatinine clearance is 90-120ml/min.
• Factors affecting serum Creatinine are Renal diseases,
glomerulonephritis, congestive cardiac failure (CCF) renal failure, and
older people.
The GFR is the best measure of glomerular function.
Normal GFR is approximately 125 mL/min
30.
Madan Bhandari Academyof Health Sciences
Conti…
When GFR decreases to 30% of normal moderate renal insufficiency. Patients
remain asymptomatic with only biochemical evidence of a decline in GFR
As the GFR decreases further severe renal insufficiency characterized by
profound clinical manifestations of uremia and biochemical abnormalities, such
as acidemia; volume overload; and neurologic, cardiac, and respiratory
manifestations
When GFR is 5% to 10% of normal ESRD
Inulin clearance and creatinine clearance are used to measure the GFR.
Madan Bhandari Academyof Health Sciences
Inulin Clearance test:
• Inulin clearance is a method of choice.
• Inulin is a polysaccharide of fructose, which is filtered by the glomerulus, but not
reabsorbed, secreted or metabolically altered by the renal tubule.
• The value of GFR as measured by inulin clearance is 125 mL/min. About 100 mL of sterile
10% solution of inulin is given as slow intravenous drip within 2 hours.
• Urine specimen formed during this period is collected totally. Blood sample is taken at the
middle of the test. Inulin is estimated by resorcinol giving a red color.
Disadvantages:
Inulin needs intravenous administration. & also technical difficulty for the analysis
33.
Madan Bhandari Academyof Health Sciences
Urea clearance test:
• The urea clearance is less than GFR, because 40% of the filtered urea is
normally reabsorbed by the tubules.
Procedure:
• Allow the patient to have a normal breakfast. At 9 am,give a cup of water &
the patient is instructed to void the bladder, and urine is discarded. At 10 am
bladder is completely emptied & volume of urine is measured & the urine urea
is measured. & blood sample should be taken for, estimation of Blood urea.
34.
Madan Bhandari Academyof Health Sciences
Conti…
• UC= U×V U-mg of urea per ml of urine.
P P-mg of urea per ml of plasma
V-ml of urine excreted per minute.
Normal values:
Normal values- 75 ml/min.
Clinical:
The values fall progressively with failing renal function.
35.
Madan Bhandari Academyof Health Sciences
Cystatin C as a Filtration Marker
• It is a marker which has advantages over serum creatinine. Cystatin C is a
13 kD (120 amino acids) non-glycosylated protein.
• Normal blood level of cystatin is 0.8 to 1.2 mg/L. It is seen in high
concentrations in biological fluids, such as breast milk, tears, saliva and
semen.
• It is expressed in virtually all organs of the body. It is the most abundant
extracellular Cysteine protease inhibitors.
36.
Madan Bhandari Academyof Health Sciences
Estimated GFR
This is a simple technique for estimating CC & there by GFR, by using Creatinine
value.
Formula- Cockcroft-Gault equation.
Ccr= (140 - age in yrs) × wt in kg(0.85 in females)/ 72 × creatinine value in mg/dl.
By MDRD- new formula(modification of diet in Renal disease)
eGFR ml/min/1.73m²= 186 ×( creatinine /88.4)-1.154×(age) 0.203×(0.742 In
females).
37.
Madan Bhandari Academyof Health Sciences
MARKERS OF GLOMERULAR PERMEABILITY
• The glomerulus act as selective filter for the blood passing through its capillaries.
• Passage of macro molecules is restricted based on their shape and size.
• Molecules such as urea, glucose, creatinine and electrolytes can pass easily but
molecule like Albumin is retained.
• Low MW protein freely get filtered, reabsorbed and catabolized by renal cells.
• Normal urinary protein excretion is less than 150mg/24 hrs, mostly made up of
Tamm Horsfall glycoprotein.
38.
Madan Bhandari Academyof Health Sciences
• The protein estimations are done by immunochemical methods.
• The appearance of significant quantities of protein like albumin indicates
increased glomerular permeability.
• Proteinuria
39.
Madan Bhandari Academyof Health Sciences
• It may be of the following types:
a. Increase in filtered load due to glomerular damage and vascular permeability—This is
called glomerular proteinuria.
b. Increased circulating concentration of low molecular weight proteins—(Overflow
proteinuria).
c. Decrease in absorptive capacity
40.
Madan Bhandari Academyof Health Sciences
Proteinuria
• They may be of following types:-
1. Glomerular proteinuria
2. Micro-albuminuria
3. Overflow Proteinuria
4. Tubular proteinuria
5. Nephron loss Proteinuria
6. Urogenic Proteinuria
41.
Madan Bhandari Academyof Health Sciences
Overflow proteinuria
• When small MW proteins are increased in blood, they overflow into
urine which is called Overflow Proteinuria.
• Eg Hb having MW 67,000 can pass through Normal glomeruli and
therefore if it exists in free form ( hemolytic conditions), Hb can appear
in urine (hemoglobinuria).
• Myoglobinuria in case of Muscle injury
42.
Madan Bhandari Academyof Health Sciences
Conti…
• In about 20% of cases of Multiple Myeloma( plasmacytoma), the light
chains of Ig are produced abnormally. Being Smaller MW, they are excreted
in urine. These are called Bence-Jones Proteins.
• When the urine is heated, at 45 degrees they start precipitating, at 60 degrees
there is maximum precipitation, at 80 degrees these start re-dissolving and at
100 degree, a clear solution is formed.
• The precipitate re-forms on cooling. Also detected by immuno-precipitation.
43.
Madan Bhandari Academyof Health Sciences
Test for Tubular functions:
• It is dependent upon,
- Adequate GFR,
- Renal plasma flow,
- Tubular mass,
- Healthy tubular cells,
- Antidiuretic hormone(ADH).
The urinary specific gravity & Osmolality are use to measure the concentrating & diluting ability of the
tubules.
44.
Madan Bhandari Academyof Health Sciences
Specific gravity of Urine
• Specific gravity depends on solute concentration and osmolality depends
on the number of osmotically active particles.
• In proteinuria Specific gravity is elevated.
45.
Madan Bhandari Academyof Health Sciences
Measurement of Osmolality
• The osmolality of urine vary widely (60milliosmol/kg to 1200milliosmol/kg)
• A random urine sample may have osmolality around 600milliosmol/kg and
it increases to 850milliosmol/kg after 12 hr fluid restriction.
• Simultaneously plasma and urine osmolality is measured and their ratio is
calculated.
• Normal ratio 3-4.5
• Normal plasma Osmolality 285-300milliosmol/kg
46.
Madan Bhandari Academyof Health Sciences
Urine concentration test
• Also called as Fluid deprivation test.- Fluid intake is withheld for 15 hours.
• The first urine sample in the morning is collected,& osmolality or Specific
gravity is measured.
• If it exceed osmolality 850mosmol/kg or sp. gravity 1.025, then the renal
concentrating is normal
• If the range is low, means the renal concentrating ability is impaired. Is either
due to, Tubular defect or decreased secretion of ADH.
47.
Madan Bhandari Academyof Health Sciences
Urine Dilution test
• The patient is not allowed to drink any water after midnight.
• Bladder is emptied at 7 am & water load is given 1200 ml over the next
30 min.
• Hourly urine samples are collected for the next 4 hours separately.
• Volume, sp. gravity, osmolality of each sample is measured.
48.
Madan Bhandari Academyof Health Sciences
Conti…
• Normal person will excrete almost all the water load within 4 hours.&
Sp. gravity of at least one sample shoud fall to 1.005 & osmolality to 50
mosmol/kg.
• More sensitive and less harmful than concentration test.
49.
Madan Bhandari Academyof Health Sciences
Urine Acidification Test (metabolic acidosis)
• For this test, give ammonium chloride at a dose of 0.1g/kg. Body weight.
(oral).The ammonium chloride (NH4Cl), is dissociated into NH4+ and
Cl−.
• In the liver NH4+ is immediately converted into urea.
• Therefore Cl- ions are counter balanced by H+ to produce HCl. It is then
excreted through urine so as to produce acidification.
50.
Madan Bhandari Academyof Health Sciences
Conti…
• Urine is collected hourly. from 2-8 hrs after ingestion.
• Then pH & acid excretion of each sample is noted.
• At least one sample should have a pH 5.3 or less.
• And ammonium excretion should be 30-90 mmol/hr
51.
Madan Bhandari Academyof Health Sciences
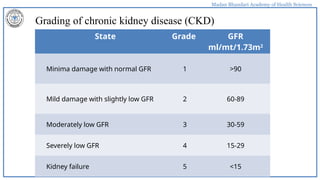
Grading of chronic kidney disease (CKD)
State Grade GFR
ml/mt/1.73m2
Minima damage with normal GFR 1 >90
Mild damage with slightly low GFR 2 60-89
Moderately low GFR 3 30-59
Severely low GFR 4 15-29
Kidney failure 5 <15
52.
Madan Bhandari Academyof Health Sciences
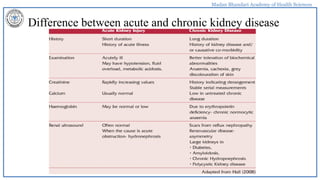
Difference between acute and chronic kidney disease
53.
Madan Bhandari Academyof Health Sciences
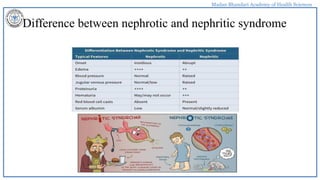
Difference between nephrotic and nephritic syndrome
54.
Madan Bhandari Academyof Health Sciences
Reference
Tietz Fundamental of Clinical Chemistry.
Textbook of Biochemistry, by DM Vasudeven.
Essentials of Medical Physiology by K. Sembulingam &
Renal system figure from Internet