Downloaded 946 times

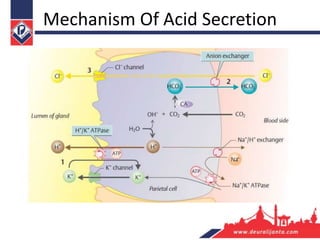
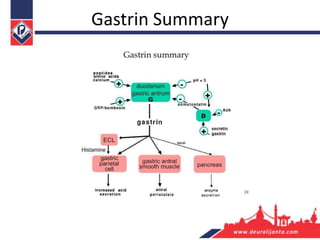
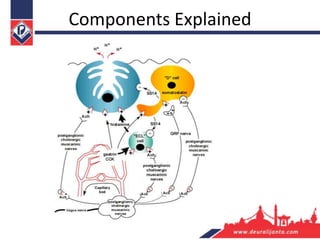

This document provides an overview of gastric acid secretion physiology. It discusses the intricate balance of stimulatory and inhibitory pathways that control acid secretion, including the cephalic, gastric, and intestinal phases. The key players in acid secretion are histamine, gastrin, acetylcholine, and somatostatin. Histamine is the major paracrine stimulator, while somatostatin is the main inhibitor. Gastrin enhances acid secretion by stimulating histamine release from ECL cells. Acetylcholine increases gastrin release and stimulates parietal cells. Prostaglandins and other factors provide autocrine inhibition of acid secretion. Pepsin secretion is closely linked to acid levels in the stomach





































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)






