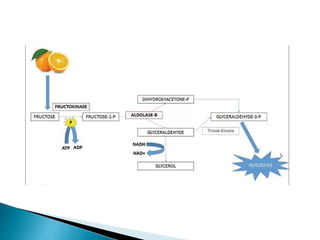
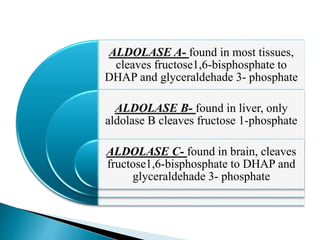
Fructose is metabolized primarily in the liver and small intestine. In the liver, fructose is converted to fructose-1-phosphate by fructokinase using ATP as energy. Fructose-1-phosphate is then cleaved by aldolase B into glyceraldehyde and dihydroxyacetone phosphate, which both enter glycolysis to generate energy. This pathway allows fructose to be rapidly metabolized and generates intermediates for glycolysis, though it requires two ATP per fructose molecule. Disorders of this pathway can cause hypoglycemia or liver failure if not treated by avoiding dietary fructose and sucrose.