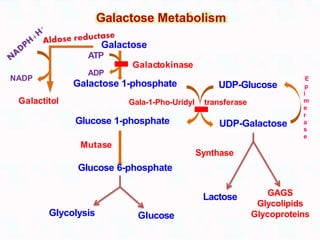
- Galactose is obtained through the diet primarily from lactose in milk and is metabolized mainly in the liver. It is converted to glucose through a series of enzymatic reactions involving galactokinase, galactose-1-phosphate uridylyltransferase, and UDP-glucose 4-epimerase.
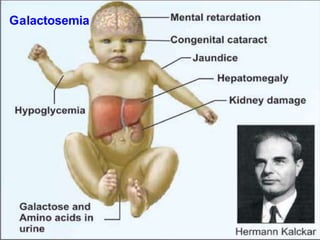
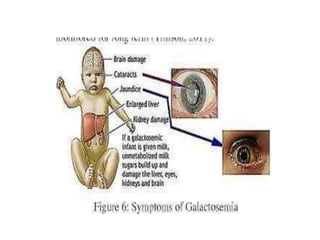
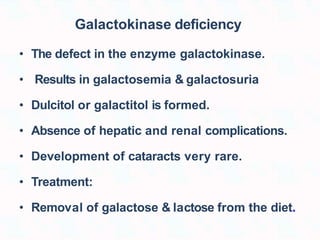
- Deficiencies of galactokinase or galactose-1-phosphate uridylyltransferase can cause galactosemia, leading to an accumulation of galactose and its metabolites in tissues and symptoms including liver damage, cataracts, and intellectual disability.
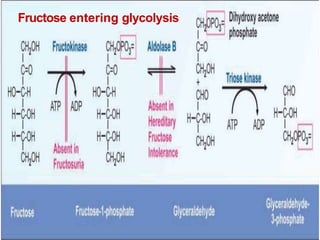
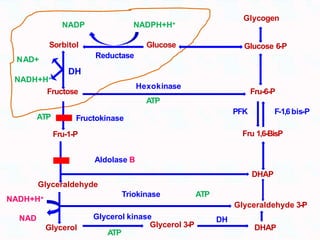
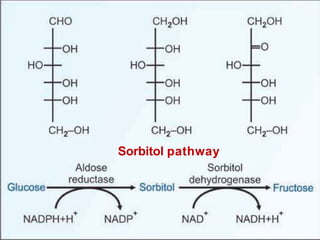
- Fructose obtained through the diet is converted to glucose mainly in the liver
















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)












