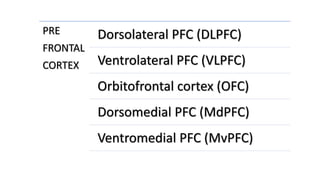
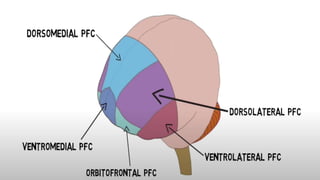
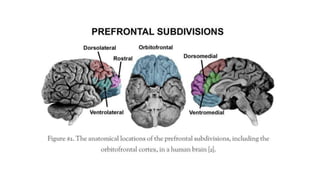
This document provides information about the prefrontal cortex. It begins with an introduction and overview of the major parts of the prefrontal cortex, including the dorsolateral, ventrolateral, orbitofrontal, and medial regions. It then describes the functions of each region and various tests that can assess prefrontal cortex functioning, such as the Wisconsin Card Sorting Test. The document concludes by discussing several disorders associated with prefrontal cortex dysfunction, such as schizophrenia, depression, and frontal lobe syndrome.


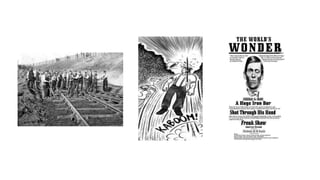



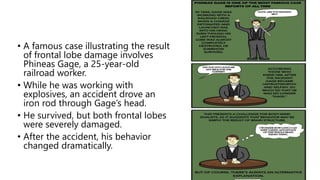
![• The case was written up by J. M. Harlow, M.D., in 1868, as follows:
[Gage] is fitful, irreverent, indulging at times in the grossest profanity
(which was not previously his custom), manifesting but little
deference for his fellows, impatient of restraint or advice when it
conflicts with his desires… His mind was radically changed, so
decidedly that his friends and acquaintances said he was “no longer
Gage” (Courtesy of Anthony A. Walsh, Ph.D.)](https://image.slidesharecdn.com/prefrontalcortex-230514143155-97186a6d/85/PREFRONTAL-CORTEX-pptx-53-320.jpg)