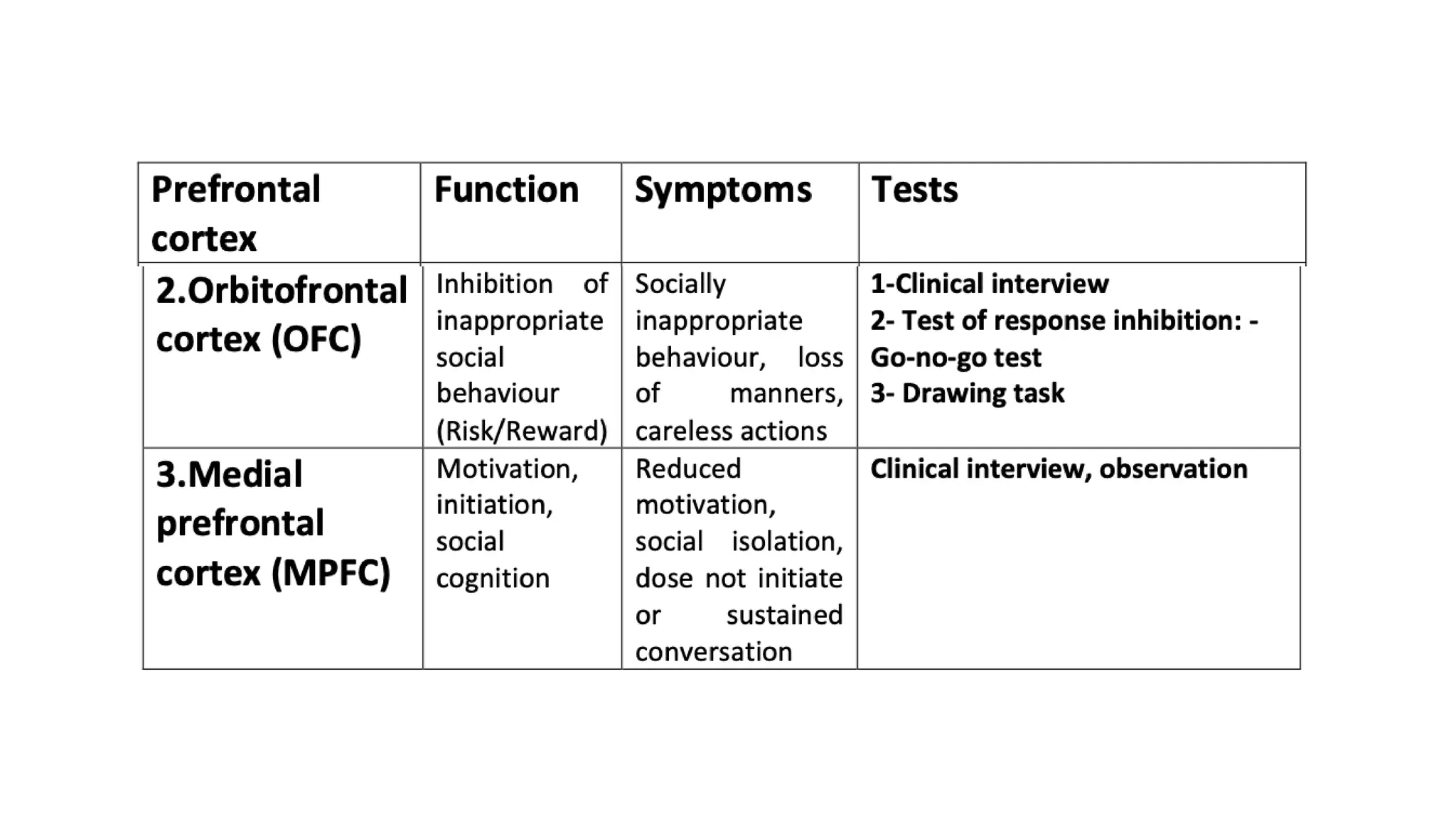
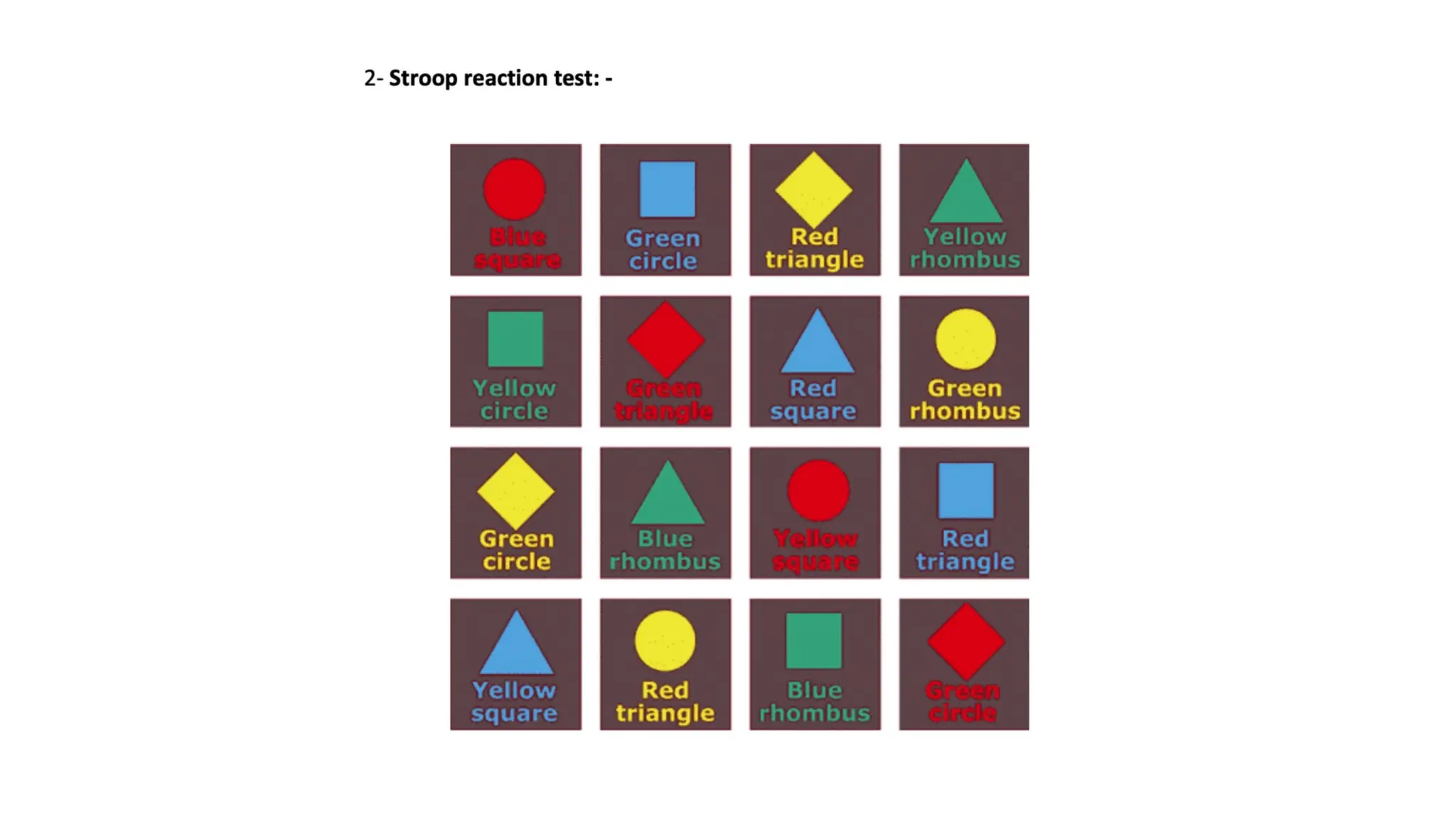
The document outlines the anatomy, functional regions, and associated disorders of the frontal lobe, detailing its location, structure, and blood supply. It describes key areas such as the primary motor cortex, prefrontal cortex, and Broca's area, along with their functions and potential consequences of lesions. Various lobar function tests for assessing frontal lobe functionality are also discussed.