Content
Micro and MacroAnatomy of cerebral hemispheres
Cerebral white matter
Neuronal networks
Vascular neuroanatomy
Neurolocalization and Hemispheric specialization
3.
Introduction
Clinical diagnosis inneurology requires recognition of impaired function,
the site of the nervous system affected and what the lesion is.
The pattern of structures is relatively constant from person to person
which makes localization possible
Lesion localization in the cerebral hemispheres relies on the understanding
of the function of different portions of the cerebral cortex.
4.
The Cerebral Hemisphere
Thepaired cerebral hemispheres derive from the telencephalon
Contains approximately 20 billion neurons spread over an area of 2.5 m2
The cortex is thrown in to folds called gyri and in between are the sulci
Its thickness varies from 4.5 mm in the precentral gyrus to 1.3 mm near
the occipital pole
5.
Why do womenmultitask better than men?
The corpus callosum is larger in women than in men and contains
more neural pathways
This is thought to make women superior in processing language,
information, emotion and cognition
The inferior-parietal lobe is larger in men and it control characteristics
that make a person more prone to mechanical and analytical thought
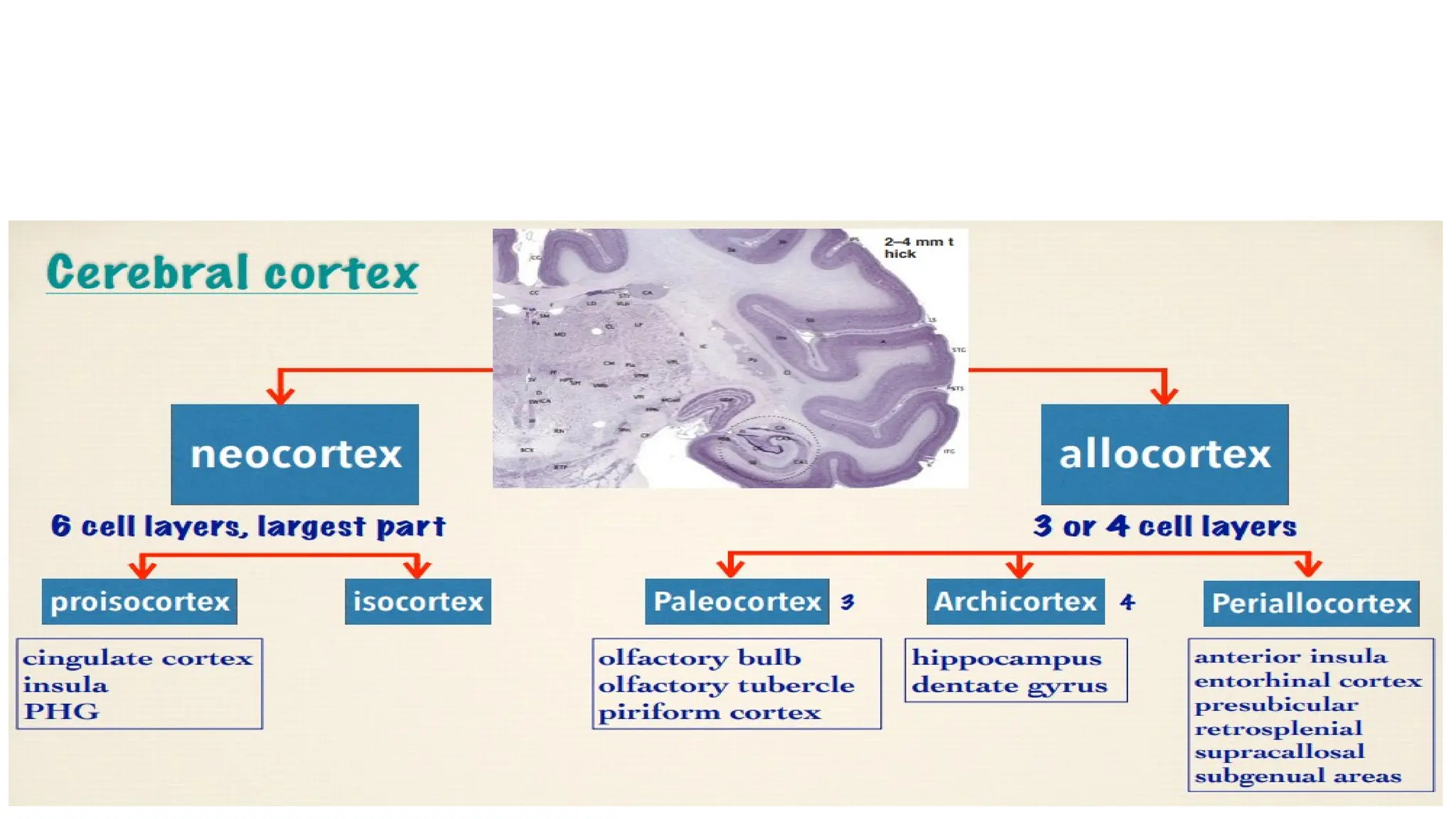
Neocortex (new cortex)- 6 layers
a. Ideotypic cortex - 1° motor and sensory cortex
b. Homotypic cortex - association areas
Mesocortex (middle cortex) - 3-6 layers - related to limbic system
a. Cingulate gyrus
b. Para hippocampal gyrus
Allocortex (other cortex) - 3 layers
a. Archicortex - hippocampal formation
b. Paleocortex – olfactory area
9.
The Gross Anatomyof the Cerebral
Hemispheres
The two hemispheres are Separated by a
longitudinal cerebral fissure
Superolateral surface are separated by two large
sulci
• Sylvian fissure
• Rolandic or central sulcus
Two imaginary lines
• From upper end of parieto-occipital sulcus to
parieto-occipital notch
• Backward continuation of the lateral sulcus
to meet the first imaginary line
10.
Covered by thingrey matter (2-4mm)
Three poles
• Frontal pole anteriorly
• Occipital pole posteriorly
• Temporal pole
Surfaces
• Superolateral surface
• Medial surface
• Inferior surface
11.
The four lobesare
Frontal lobe
Parietal lobe
Temporal lobe
Occipital lobe
Other, sometimes designated as a lobe
because their parts are interconnected
functionally
• Insula
• Limbic lobe
12.
Broadmann’s Map
These areaswere defined and
numbered by korbinian broadmann
Based on the cortical
cytoarchitectonic organisation of
neurons
Many of the broadmann’s areas
are defined on neurological
function correlated closely to
diverse cortical functions
13.
Frontal lobe
The largestof the 4 major paired
lobes of the brain, 38% of human
brain
Lateral view; central sulcus and
Sylvain fissure separates it from
adjacent lobes
Medial view; Cingulate sulcus-
separates the cingulate gyrus from
the first frontal and paracentral
gyri
Inferior view Orbital surface of the
prefrontal area
It is dividedin to 3 functional areas
• The primary motor area (area-4)
• The premotor area (areas 6, 8, 44, & 45)
• The prefrontal cortex (areas 9-12)
16.
Prefrontal cortex (BA9-12,32,45-47)
Frontal lobe anterior to premotor area
Connections: With the Hypothalamus, thalamus, limbic system, motor
areas, the temporal and occipital lobes
Has three clinically important divisions
• DLPFC(dorsolateral prefrontal cortex)
• MPC(medial prefrontal cortex)
• OFC(orbitofrontal cortex)
17.
Functions
DLPFC
Organization of tasks,execution, problem solving, personality, affect and decision
making
MPC
Important in auditory and visual associations
OFC
Connection with the limbic system, Including the amygdala
Frontal eye field control movement of the eyes to the contralateral side
Motor speech areas(Broca’s)(BA 44,45)
18.
Lesions
Stimulation
• Psedoseizure likepedaling and thrusting
• Aversive seizure
Frontal eye field
• Destructive lesions cause gaze deviation ipsilaterally
• Epileptiform activity cause gaze deviation to the contralateral side
Broca’s Aphasia
Unilateral- imitation and utilization behavior
19.
Frontal motor areas
1.Primary motor cortex(BA 4)
Contains large motor neurons (Betz cells)
giving tracts to
• Corticospinal
• Corticobulbar
Motor Homunculus
• Crossed and inverted representation of
the body according to the motor value
20.
Function
Initiation of voluntary,fine, discrete (separate) mov´t of limbs. (eg. Hands,
fingers) on opposite side
Facilitation of stretch reflex i.e Facilitation of skeletal muscle tone and
tendon jerk
Lesions
Irritative; focal seizure
Destructive ; contralateral Flaccid paralysis
Loss of deep and cutaneous reflexes in the opposite side
21.
2. Pre motor
Receivesafferents from other areas of the cortex and projects to the motor
cortex and the motor thalamus
Involved in the planning and execution of movements, particularly sequences
of movements
Some fibers descend and make up part of the extrapyramidal system
3. The SMA (Supplementary motor cortex)
consists of areas of cortex lying on the medial aspect of the hemisphere
Involved coordinating sequence of actions provided from memory
22.
Lesions
Stimulation
• Tonic posturingwith or without automatism
Destructive
• Increase in muscle tone & muscle spasticity than weakness
• Exaggerated tendon jerk
• Reappearance of primitive reflex
• Motor aphasia and apraxia
• Agraphia: failure of writing & drawing skills due to lesion to exner´s
center
23.
Q1. Why dopatients with UMNLs tend to have muscle spasticity and
increased tone?
The EPF transmit inhibitory impulses that lower muscle tone
Destruction of the secondary motor area removes the inhibitory influence,
and consequently, the muscles become spastic
Q2. What kind of plantar response do we expect with lesions in the primary
motor area
A positive Babinski´s sign in the opposite side with only dorsiflexion of big
toe due to lesion of pyramidal fibers ( no fanning occurs in other fingers
b/c extra pyramidal tracts are intact)
24.
Bilateral Frontal lobelesions
Akinetic mutism
Gait apraxia
Incontinence
Perseveration
Lack of judgement and foresight
Aspontaneity and lability
25.
Parietal lobe
The parietallobe lies posterior to the central sulcus, anterior to the occipital lobe and
superior to the temporal lobe.
Five principal parts:
• The postcentral gyrus
• The posterior portion of the paracentral lobule
• The superior parietal lobule
• The inferior parietal lobule
• The precuneus
26.
1. The primarysomatosensory cortex(S1) (BA 3, 1, 2)
Lies between the central sulcus and the postcentral sulcus
Granular cortex densely packed with stellate cells
Sensations derived from skin are appreciated in anterior part of the area and
proprioceptive sensations in posterior part of the area
If lesions occur without involving thalamus, sensations are perceived but
discriminative functions are lost
If thalamus also affected, loss of sensations in opposite side of body
29.
2. Secondary sensoryarea/ SII
Situated in post central gyrus
Receives sensory impulses from primary sensory area and thalamus
Neurons in anterior part respond to touch whereas neurons in
posterior part can be excited by touch, auditory, visual and nociceptive
stimuli
3. Sensory association areas (BA 5,7,40)
• Neurons which react to passive or active rotation of a joint or joints
• Higher association area, concerned with stereognosis
30.
4. The Precuneus
•Is an area of the cortex just anterior to the occipital lobe on the medial
hemispheric surface
• Involved in visuospatial imagery, episodic memory retrieval
31.
Lesions
Unilateral lesion( Either
Hemisphere)
•Loss of Cortical Sensations
• Loss fine touch more than pain
Hypotonia, muscle atrophy, and
pseudoataxia
• Lower quadrantanopia
Bilateral lesion:
• Severe Constructional Apraxia
• Optic Ataxia
Case-1
A 78 yearsold female presents with an acute onset of confusion, lately she
had a difficulty of doing her bill's with simple mathematical calculation, she
had a difficulty of reading a written language . She went to doctor and On
examination there is impaired right left orientation, arithmetic abilities and
finger identification
MRI shows severe foci of cortical and subcortical increased T2 signals the
most probable diagnosis is??
Temporal lobe
Situated inferiorto the lateral fissure and anterior to the parieto-occipital sulcus
Contains three gyri, separated by two sulcus
• Superior gyrus - auditory and language functions
• Middle and inferior gyri -integration of vision
Hippocampal formation
• Learning and memory
Amygdala; emotions(fear, anger…)
36.
1. Primary auditorycortex (areas 41 and 42)
The transverse temporal gyri (of Heschl)
Buried in the Sylvain fissure at the posterior end of the superior
temporal gyrus on its dorsal surface
Hearing is bilaterally represented but there is contralateral dominance
2. The auditory association cortex(Area 22)
Found immediately adjacent to the primary auditory cortex
Differentiate and interpret sounds
3. Wernicke’s speech Area (Area 22)
Posterior superior temporal area, in the dominant hemisphere
Occipital lobe
A smallpart of the dorsolateral surface of the
hemisphere
It rests on the tentorium cerebelli
It is separated on medial surface from parietal
lobes by parieto-occipital fissure
The lateral occipital sulcus, divides the lobe
into superior and inferior occipital gyrus
The calcarine fissure separates the medial
surface into the cuneus above and the lingual
gyrus below
39.
1. Primary visualcortex(BA 17)
At the lip of the calcarine
Receives primary visual impressions as Color, size, form, motion and illumination
Receives fibers from the temporal half of the ipsilateral retina and the nasal half of the
contralateral retina
Lesions
• Stimulation- visual hallucination, scotoma and flash of lights
• Destructives- visual field defect, usually macular sparing hemianopia
• Bilateral lesions- Cortical blindness
Bilateral hemianopia, scotoma
Anton's hallucination syndrome
40.
2. Visual AssociationArea – (Area18 & 19)
Recognition and identification of objects and store visual memories
Area 18- receive stimulus from the primary visual cortex
Area 19- connects with the entire cortex
Lesions- Contralateral disconnection syndrome, visual inattention
Unable to localize himself or objects in space
3. Fusiform and lingual gyri
Color vision and face recognition
Lesions- Prosopagnosia
41.
The Limbic lobe
Sometimesconsidered a separate lobe of the brain, because of its function
than its anatomy
A ring of cortex on the medial aspect
of each cerebral hemisphere and includes
• The cingulate gyrus
• The Para hippocampal gyrus
• The hippocampus:
• The mammillary bodies (part of the hypothalamus);
• The anterior nucleus of the thalamus;
42.
Functions
• This systemparticipates in the control of autonomic function, arousal,
motivated behavior, emotion, learning, and homeostasis
Lesions
• A disturbance in this function is known as an amnestic state. And it can be
Anterograde, retrograde or global.
Cerebral White Matter
•A central core of white matter that forms the bulk of the cerebrum
and represents fiber tracts
• Supported by Neuroglia, carrying information destined for the cortex
and Cortical responses to other regions of the CNS
• There are three types of fibers based on their orientation
45.
Association fibers
• Connectone area of cerebral cortex with another area in the same
hemisphere
Commissural fibers,
• Connect areas of the cerebral cortex in opposite hemispheres
• Main ones are Corpus callosum, anterior commissure and the hippocampal
commissure
Projection fibers
• Project to deep structures, like the thalamus
47.
Q. What istheir clinical importance?
Characteristics of white matter lesions are
• Weakness
• Spasticity
• Visual field deficits
• “Pure” motor syndromes
• Urinary incontinence
Lesions cause symptoms that are referable to the cortical region giving rise
to the white matter tract involved
48.
Neural networks
Five anatomicallydefined large-scale networks are most relevant to clinical
practice:
1. Perisylvian network for language,
2. Parietofrontal network for spatial orientation,
3. Occipitotemporal network for face and object recognition,
4. Limbic network for retentive memory, and
5. Prefrontal network for the executive control of cognition and comportment.
Aphasia
• Aphasia isa defect in language
processing caused by damage to
any one of the neural network
component
• In ~ 90-95% of right-handers and
60-70% of left-handers, aphasia
occurs only after lesions of the left
hemisphere.
52.
1. Wernicke’s Aphasia
Markedlyimpaired comprehension, Impaired naming and repetition
Normal fluency, prosody, and grammatical structure.
Writing and Reading: similarly affected
Prognosis for recovery of language function is guarded
2. Broca’s Aphasia
Intact comprehension
Decreased fluency, Impaired repetition
Marked naming difficulties
53.
3. Conduction Aphasias
Normal fluency and normal comprehension, but impaired repetition
Interruption at the arcuate fasciculus or other pathways in the vicinity of the
supramarginal gyrus that connect Wernicke’s area to Broca’s area
4. Transcortical Aphasias
Resemble Broca’s, Wernicke’s, and global aphasias, except that repetition is
spared
Classic cause: watershed infarcts
Three types; Motor (non fluent) type, Sensory (fluent) aphasia and mixed
54.
6. Global Aphasia
•The combined dysfunction of Broca’s and Wernicke’s areas
• All modalities of speech are impaired
• from strokes that involve the entire MCA distribution in the left hemisphere
6. Subcortical Aphasia
• Subcortical components of the language network including Thalamus and
Basal ganglia
• Combinations of deficits but rarely fit the specific patterns
56.
Do we expectAphasia in right hemispheric lesion???
First, right-handed patients occasionally become aphasic after right
hemisphere strokes, a phenomenon called crossed aphasia.
Second left-handed patients may have right hemisphere language dominance
Third, even right-handed persons with typical left hemisphere dominance for
language have subtly altered language function after right hemisphere
damage
57.
Role of thenondominant hemisphere in language?
• Important in both the recognition and the production of the affective
elements of speech.
• Lesions: difficulty judging the intended expression imparted by a particular
tone of voice, or they may have difficulty producing emotionally
appropriate expression in their own voice.
• In lesions of the dominant hemisphere, callosal connections may allow the
nondominant hemisphere to take over some functions of the damaged
areas and to participate in at least partial recovery
58.
2. The prefrontalnetwork for Attention &
Behavior
Prefrontal network:
• Prefrontal Cortex (motor-premotor, dorsolateral , medial , and
orbitofrontal components)
• Subcortical Structures (the head of the caudate and the dorsomedial
nucleus of the thalamus).
Important role: integration of thought with emotion & motivation.
59.
Lesions
Frontal AbulicSyndrome (DLPFC); loss of initiative, curiosity, creativity,
emotional blandness, apathy and lack of empathy.
Frontal Disinhibition Syndrome (medial/orbitofrontal): severe
impairments of judgment, insight, foresight, and the ability to mind
rules of conduct.
Fontal release signs (grasping, sucking)
These syndromes tend to arise almost exclusively after bilateral lesions.
60.
Phineas Gage (1823–1860)
Railroadconstruction man,
Sustained metal injury with
accidental frontal lobectomy.
He became unreliable, with
temperament changes
hypesexuality, poor social
interaction but with preserved
intellectual function
61.
3. The ParietofrontalNetwork For Spatial
Orientation
Network for directed attention to extra personal
space includes:
• Cortical components
The posterior parietal lobe
Frontal eye fields
Cingulate gyrus and their connections
• Subcortical components : striatum and thalamus
Lesions
• Hemispatial neglect,
• Simultanagnosia and object finding failures.
62.
Q. Why doesright hemispheric lesions cause Hemineglect??
The right hemisphere directs attention within the entire extra personal
space, whereas the left hemisphere directs attention mostly within the
contralateral right hemi space
64.
Case -2
A 68years old male who had a difficulty of finding where the door is and
where the wall ends, after he wakes up from sleep. He first thought he did
not have a good night sleep he stretch out to find his telephone but couldn’t
find it out, one of his family members point it out and it was right next to
him where he left it the eye doctor told him that his vision is quite normal
despite the fact he hardly find the way out form the doctors office what is
happening to the patient ??
65.
Balint’s Syndrome
Bilateral involvementof the network for spatial attention, especially its
parietal components
Components of Balint’s syndrome are:-
1. Oculomotor apraxia
2. Optic ataxia, and
3. Simultanagnosia
Etiology: CVA, hypoglycemia, sagital sinus thrombosis, Alzheimer’s disease
66.
Case 3
A 65year old male patient come to you with complaint of sudden failure to
recognize his Son by looking at his face whom he recognized later as he
conversed to him. His Ophthalmologist confirmed that he doesn’t have eye
problems. He still complains that he recognizes his son only hearing his
voice and looking his clothing.
67.
4. Occipitotemporal network
Prosopagnosia
patientsare unable to recognize people by looking at their faces
The usual lesion location is the bilateral inferior occipitotemporal cortex,
also known as the fusiform gyrus
Achromatopsia
A central disorder of color perception.
Others- Micropsia, Macropsia, Metamorphopsia, Visual reorientation:
68.
5. The LimbicNetwork for Memory
Includes
• Limbic and paralimbic areas
• The anterior and medial nuclei of the thalamus,
• The medial and basal parts of the striatum, and
• The hypothalamus
Function
• Memory
• Immediate (working, Short-term (recent) and Long-
term (remote) memory
Disturbance
• Amenesia
• Could be ;Retrograde amnesia, Anterograde amnesia
or Confabulation
The arterial supplyis derived from the anterior circulation provided by
the bilaterally paired internal carotid arteries, as well as by the posterior
circulation provided by the bilateral vertebral arteries
These anterior and posterior circulations meet in an anastomotic ring
called the circle of Willis, from which all major cerebral vessels arise
The main arteries supplying the cerebral hemispheres are the anterior,
middle, and posterior cerebral arteries.
72.
ACA
Supply – frontalto anterior
parietal lobe area
Lesions
• Contralateral weakness leg more
than the arm or face with cortical
sensory loss
• transcortical motor aphasia
• contralateral neglect
• grasp reflex, impaired judgment,
flat affect, apraxia, abulia, and
incontinence
• “alien hand syndrome”
73.
MCA
Supply the dorsolateralcortex
Lesions are more common than ACA
or PCA areas
• Contralateral weakness arm and face
more than leg with cortical sensory loss
and gaze preference toward the side of
the lesion
• global aphasia, contralateral homonymous
hemianopia
• hemineglect, apraxia and anosognosia
74.
PCA
Supply inferior andmedial temporal
occipital lobe
Infraction typically cause a
contralateral homonymous
hemianopia
Also cause visual field defects, color
anomia and paresthesia without any
motor findings
Alexia without agraphia
Watershed zones
Regions betweencerebral arteries in both the ACA–MCA and MCA–PCA
zones
A sudden occlusion of an internal carotid artery or a drop in blood pressure
in a patient with carotid stenosis can cause an ACA–MCA watershed infarct
Infarcts can produce proximal arm and leg weakness (“man in the barrel”
syndrome), transcortical aphasia syndromes
MCA–PCA watershed infarcts can cause disturbances of higher-order visual
processing
77.
VASCULAR NEUROANATOMY
VEINS
• Thesuperficial veins drain
mainly into the superior sagittal
sinus and the cavernous sinus,
while the deep veins drain into
the great vein of Galen then
reaches the internal jugular
veins.
• Sagittal sinus thrombus and
other venous thrombus are the
common conditions
78.
Principles of CerebralLocalization and
Lateralization
Q. How are cortical lesions different from sub-hemispheric lesions?
Neuroplasticity and redundant pathway
Extensive neural networks
• The result is:
Less pronounced deficits with lesions caused a major motor or
sensory disturbance if occurs in the subcortical structures
Single lesions may be clinically silent and become symptomatic when
additional lesions impair the function of the network
79.
Cortical vs. subcorticallesions can sometimes be differentiated clinically
based on the absence or presence of so called cortical signs
These include
• Aphasia
• Neglect
• Seizures
• Homonymous visual field defects and
• Cortical sensory loss
However, each of these deficits can be seen in some cases of subcortical
lesions as well
80.
Case -4
A 23-year-oldwoman with a 4-year history of epileptic attacks visited
her neurologist. Her families described one of her attacks. For a few seconds
before the convulsions began, the patient would complain of an unpleasant
odor, similar to that encountered in a cow shed. This was followed by a shrill
cry as she fell to the floor unconscious. Her whole body immediately became
involved in generalized tonic and clonic movements.
81.
Anatomic location Generalcharacteristics of seizures
Frontal lobe
Usually occur several times per day, short in duration, during sleep.
Complex gestural automatisms is common at onset. Tonic/postural manifestation is prominent.
Occipital lobe
Usually simple partial and secondarily generalized seizures.
include visual symptoms that are contralateral to cortex:
Positive visual manifestations include sparks, flashes, and Negative visual manifestations include scotoma,
hemianopsia, and amaurosis.
Parietal lobe
Most are simple partial but can secondarily generalize.
In the dominant parietal lobe, language is often involved.
Sensory features: Positive symptoms include tingling and electric feeling.
Negative symptoms include numbness, absent body part, and asomatognosia.
Temporal lobe
Simple partial seizures: autonomic/psychic symptoms and sensory phenomena: olfactory, auditory, and
(most commonly) rising epigastric sensation. Complex partial seizures: alteration in consciousness with
behavioral arrest, often followed by oroalimentary or hand automatisms.
Postictal confusion is usually followed by amnesia of the event.
Clues to anatomic location of a seizure
82.
Hemispheric Specialization
Many basicsensory and motor functions in the brain are distributed
symmetrically
For unknown reasons, however, there are marked asymmetries in
several brain functions
Cerebral dominance is related to handedness and anatomic
differences between the hemispheres
83.
Handedness
• The mostobvious asymmetry in cerebral function is handedness.
• Approximately 90% of the population is right-handed
• Lesions of the dominant hemisphere therefore are more commonly
associated with apraxia, a disorder of formulating skilled movements
Language
• Another well-known example of hemispheric specialization.
• The left hemisphere is dominant for language in over 95% of right-
handers, and in over 60 to 70% of left-handers
86.
Anteroposterior Organization
In additionto left versus right, brain functions are also organized along the
anterior to posterior axis
More posterior regions are sensory and more anterior regions are motor
• The posterior parietal and temporal association cortex are more
involved in interpreting perceptual data and assigning meaning to
sensory information
• The anterior frontal association cortex is more important for planning,
control, and execution of actions
87.
References
Dejong’s the neurologicexamination, 8th
edition
W. Brazis, Localization in clinical neurology, 6th
edition
Snells clinical neuroanatomy,7th
edition
Grays the anatomic basis of clinical practice, 39th
edition
Blumenfeld Neuroanatomy through clinical cases, 2nd
edition
#29
The sensory association areas are essential for appreciation of similarities and differences, interpretation of spatial relationships and two-dimensional qualities, evaluations of variations in form and weight, and localization of sensation.
#31 Overactivity of these areas causes minimal symptoms, for example, vague paresthesias or hyperesthesias on the opposite side of the body.
Destructive lesions affect mainly the gnostic (knowing, recognition) aspects of sensation. Simple appreciation of primary sensations remains, but associative functions are impaired.
THIS area has many connections with other sensory areas of the cortex. It is believed that its
main function is to receive and integrate different sensory modalities.
For example, it enables one to recognize objects placed in the hand without the help of vision. In other words, it not only receives information concerning the size and shape of an object but also relates this to past sensory experiences; thus, the information may be interpreted, and recognition may occur.
A quarter placed in the hand can be distinguished from a dime or a nickel by the size, shape, and feel of the coin without having to use one’s eyes
Loss of temperature more than pain, Loss of Joint sense and Position more than vibration
ataxia in which patients have difficulty completing visually guided reaching tasks in the absence of other sensory cues. Patients with isolated optic ataxia have intact visual fields, stereoscopic vision, oculomotor control, proprioception, motor abilities and cerebellar function, excluding other causes of ataxia with reaching
#32 anosognosia”: denial of hemiplegic side / this side of the body is “strange
Alexia.inability to understand writing
#34 Calculations. Can the patient do simple addition, subtraction,?
Finger agnosia. name and identify each digit
Agraphia. write their name and a sentence
#36 if u peel uncus u will get Amygdala , which is a collection of neuronal cell bodies(forming amygdaloid nuceli
#37 Complex partial seizures with automatism…
Wernike- words cant be understood tough hearing is not impaired
Kluver Bucy syndrome-usually seen in animals, a rare d/o with loss of fear, rage, visual agnosis, hypersexuality memory loss
#39 All of its functions are concerned either directly or indirectly with vision
#41 The cingulate gyrus lies just above the corpus callosum.
The parahippocampal gyrus begins at the isthmus of the cingulate and runs to the temporal tip, lying between the collateral sulcus and the hippocampus
It curls around the hippocampal fissure to form the uncus.
#43 6 primary fields receiving thalamo-cortical relays
somatosensory, motor, visual, auditory, gustatory, vestibular
Understanding the functions of these various primary fields will aid in localization of cortical deficits
Primary gustatory cortex: (Area 43).
6. Primary vestibular cortex: Area 24
Integrates somatosensory, visual, auditory and motor information to control head/body position
#45 Projecting
Efferent– corona radiata fibers converge to form the internal capsule, becoming the cerebral peduncle below the thalamus
Afferent – all ascending sensory tracts (except olfaction) end in the thalamus,and are relayed via thalamo-cortical projections
#48 Most cortical functions are coordinated by intersecting large-scale neural networks that contain interconnected cortical and subcortical components.
Individual anatomic sites within a network display a relative (but not absolute) specialization
#49 Language formation…heard info through the auditory cortex and written and sign language with in the visual cortex receive the primary info, then sent to wernikes area, matched with stored vocabulary, language comprehension is achieved, the arcuate fasiculus transmit it to brocas area, responsible for production of speech, output from brocas sent to to the motor cortex which controls muscles of speech
#57 Aprosodia
Inappropriate melodic stress and intonation
Damage to right hemisphere perisylvian area;
“he is clever!” Vs “he is clever?”
#58 Similarly, lesions of the frontal lobes produce highly variable behavioral syndromes, many of which seem contradictory even within a single patient
#59 Disruption of a variety of attention-related functions
Working memory, Concentration span, reasoning, Mental flexibility.
#61 Simultagnosia: deficits in the ability to integrate visual information in the center of gaze with more peripheral information
#62 Unilateral left hemisphere lesions do not give rise to much contralesional neglect since the global attentional mechanisms of the right hemisphere can compensate for the loss of the contralaterally directed attentional functions of the left hemisphere
#63 He thinks he has shaved his whole face
Damage of the right parietal lobe
visual target cancellation
#65 oculomotor apraxia: visual inattention
optic apraxia: failure to reach an object
simultagnosia: unable to identify different items
#67 Bilateral lesions in the occipitotemporal cortex.
disruption of relay of visual perception to other multimodal areas of the cerebral cortex
bilateral infarctions in the territory of the PCA.
Achromatopsia
Patients cannot name, point to, or match colors presented visually.
They can, however, name the appropriate color for an object described verbally
#68 Memory stages and their Localization
Immediate (Working) Memory
Dorsolateral prefrontal cortex
Short-term( recent) memory
Hippocampus and parahippocampal areas of the MTL for both storage and retrieval
Long-term (Remote) memory
Once memory is well stored in the neocortex, it can be retrieved without use of the hippocampal system
#70 The anterior cerebral arteries (ACAs) and middle cerebral arteries (MCAs) are the terminal branches of the internal carotid arteries. The anterior cerebral arteries anastomose anteriorly at the anterior communicating artery (AComm). The anterior and posterior circulations are linked to each other via the posterior communicating arteries (PComms), which connect the internal carotids to the posterior cerebral arteries, thereby joining the ante-
#73 . Infarcts and ischemic events are more common in the middle cerebral artery than in the anterior or posterior cerebral arteries, at least in part because of the relatively large territory supplied by the middle cerebral artery. MCA infarcts occur in the following three general region
Large MCA territory infarcts often have a gaze preference toward the side of the lesion (see Figures 13.14 and 13.15), especially in the acute period, shortly after onset
#76 when the blood supply to two adjacent cerebral arteries is compromised, the regions between the two vessels are most susceptible to ischemia and infarction
ACA–MCA watershed infarct, since the MCA and ACA are both fed by the carotid
In addition to watershed infarcts between the superficial territories of different cerebral vessels, watershed infarcts can also occasionally occur between the superficial and deep territories of the MCA
#77 It has both superficial and deep territories
Venous thrombosis can also occur less commonly in other intracranial venous sinuses, in the deep cerebral veins, or in a major cortical vein, leading to infarcts or hemorrhage in the territories of these vessel
#78 Cortical plasticity results in a more complete recovery from elementary neurologic deficits, such as weakness or numbness, although more complex motor or sensory deficits may remain
#81 Although seizure type does not reliably distinguish seizures caused by a tumor from those with other etiologies, clinical ictal characteristics, such as focal clonic activity, may suggest that seizure onset is occurring in a focal region and an associated lesion must be excluded.
Clinical seizure semiology provides clues for the region of ictal onset and its potentially associated focal lesion. The International League against Epilepsy has described seizure syndromes according to anatomic location:
#83 The degree of asymmetry in manual dexterity varies, but most individuals are remarkably clumsy in performing tasks such as writing or closing buttons with the nondominant (usually left) hand
Although each hemisphere controls simple movements of the contralateral limbs, skilled complex motor tasks for both right and left limbs are programmed mainly by the dominant, usually left, hemisphere






























![Non-Dominant [Right]
• Unilateral anosognosia
• Amorphosynthesis: hemi-neglect,
dressing apraxia
• Visual inattention
Dominant [Left]
• Bilateral Asomatognosia
• Bilateral Astereognosis
• Tactile Agnosia
• Bilateral Ideational Apraxia
• Alexia with agraphia](https://image.slidesharecdn.com/seminaroncerebralneurolocalization-250509155940-fcd1c26b/75/Seminar-on-Cerebral-Neurolocalization-pptx-32-2048.jpg)