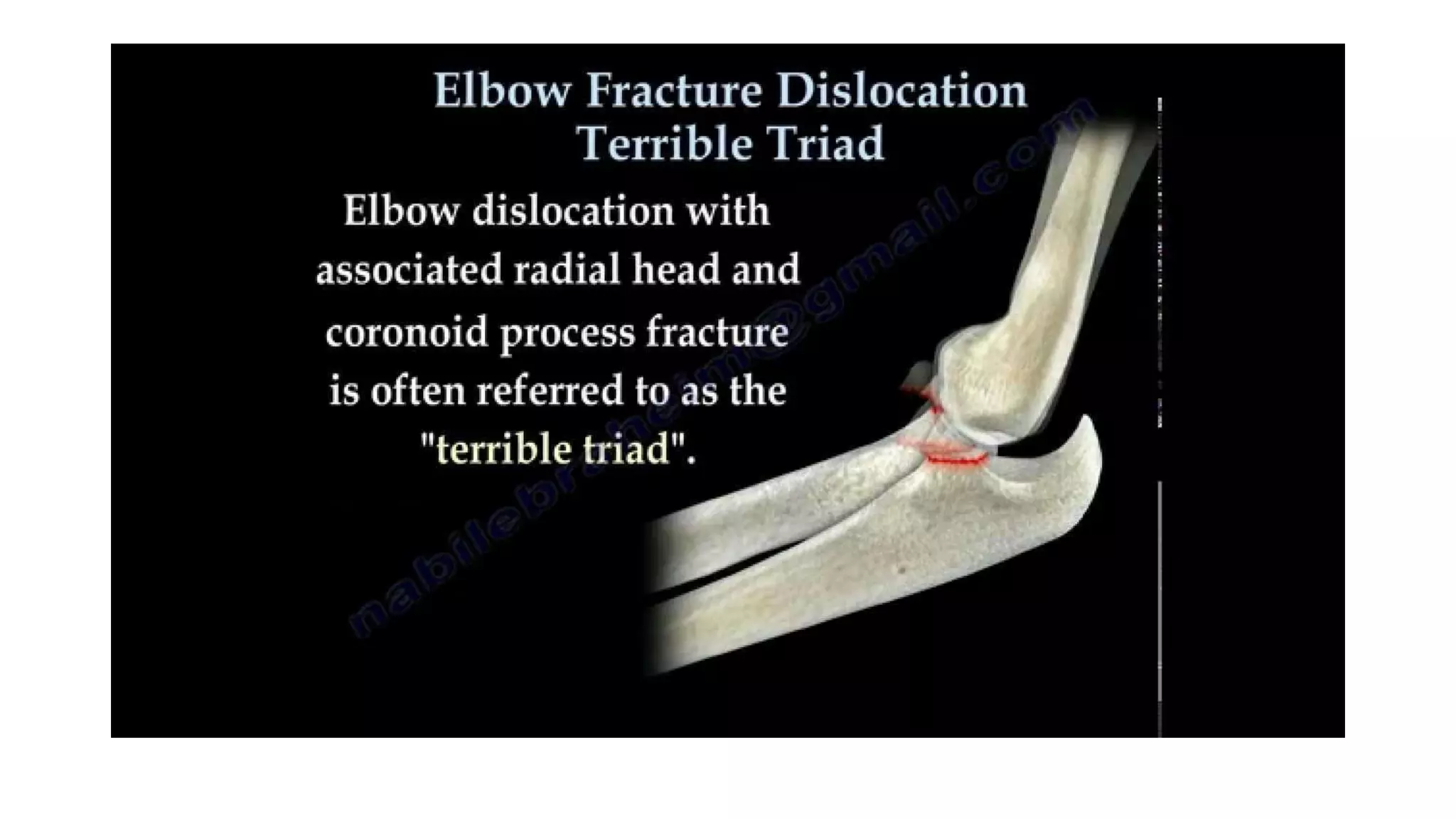
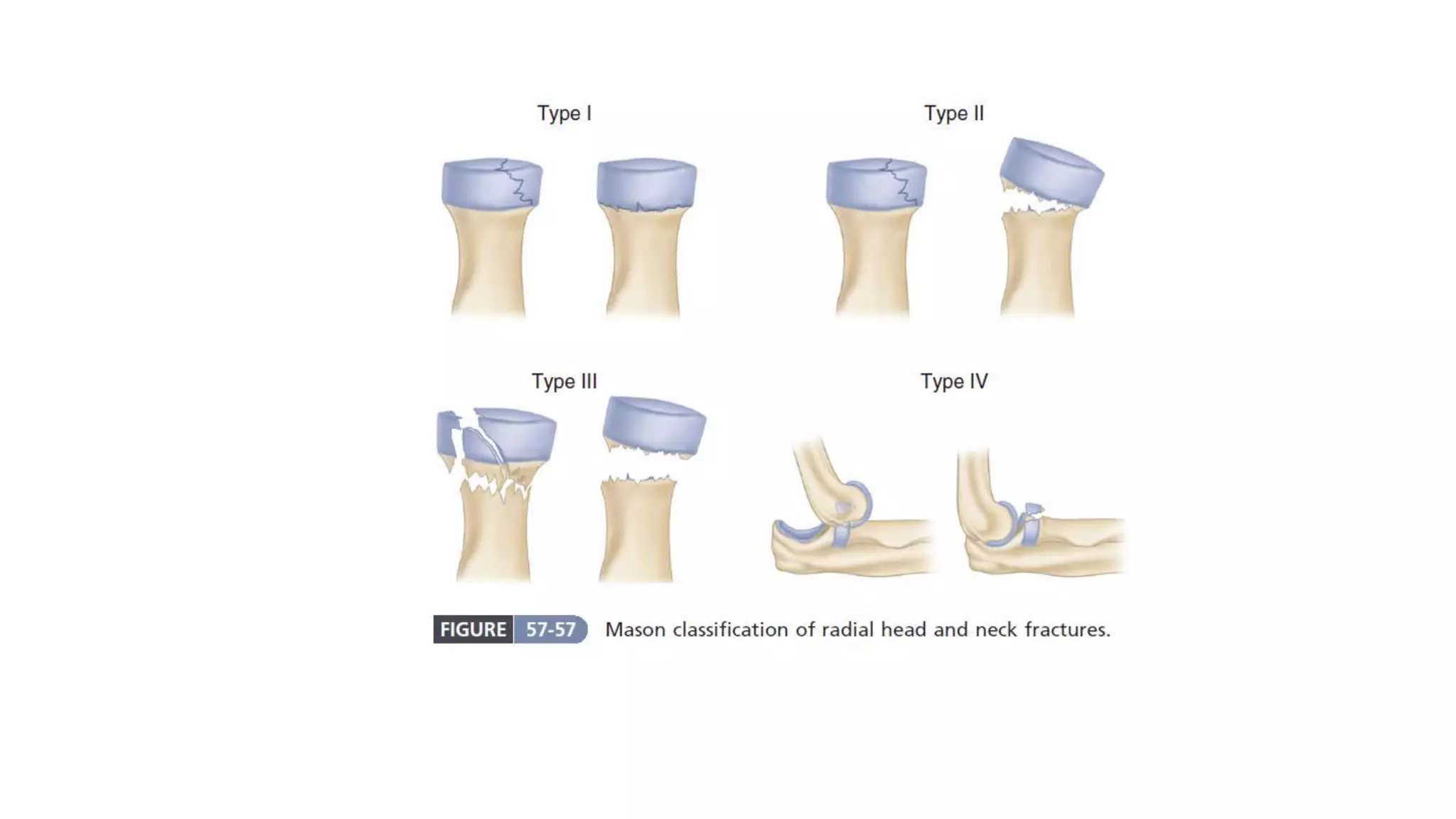
Radial head fractures are common elbow injuries that can range from undisplaced partial fractures to comminuted fractures. They are often caused by falls onto the elbow or outstretched hand. Treatment depends on the Mason classification and may involve closed reduction, open reduction with screws or plates, or fragment removal. The goal is a pain-free range of motion. Postoperative care involves splinting followed by gradual exercises over 3-4 weeks.