Downloaded 43 times
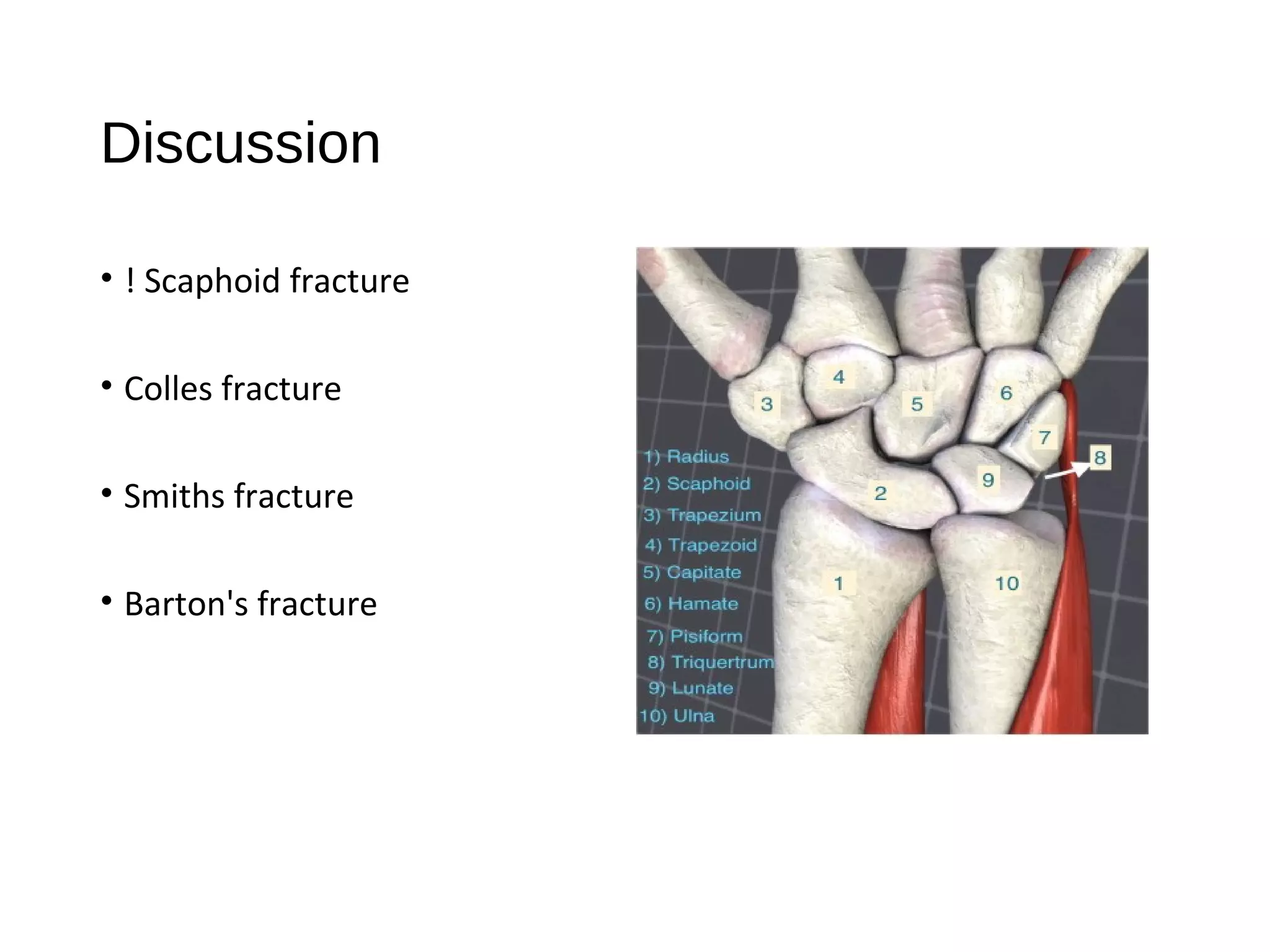
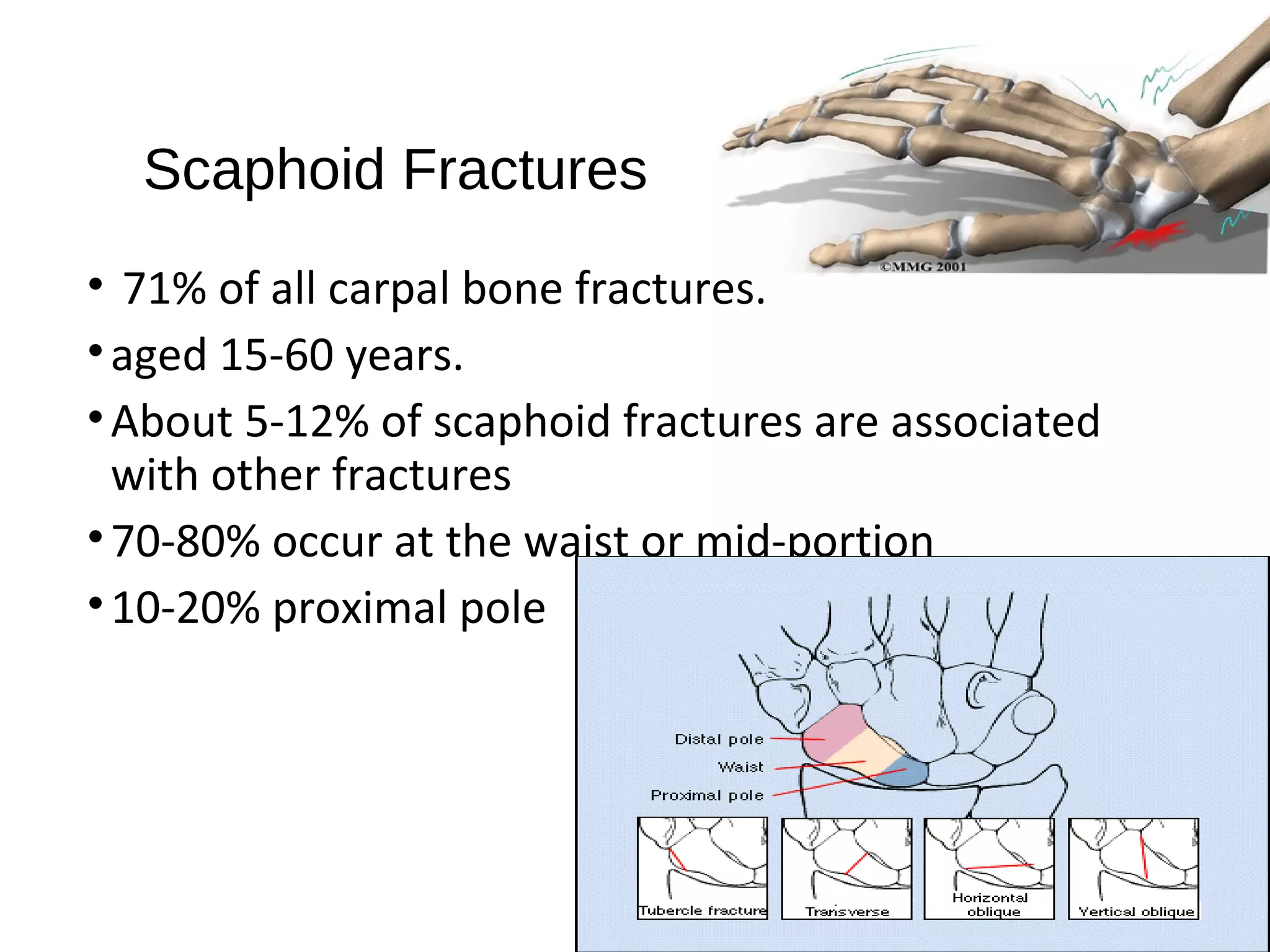
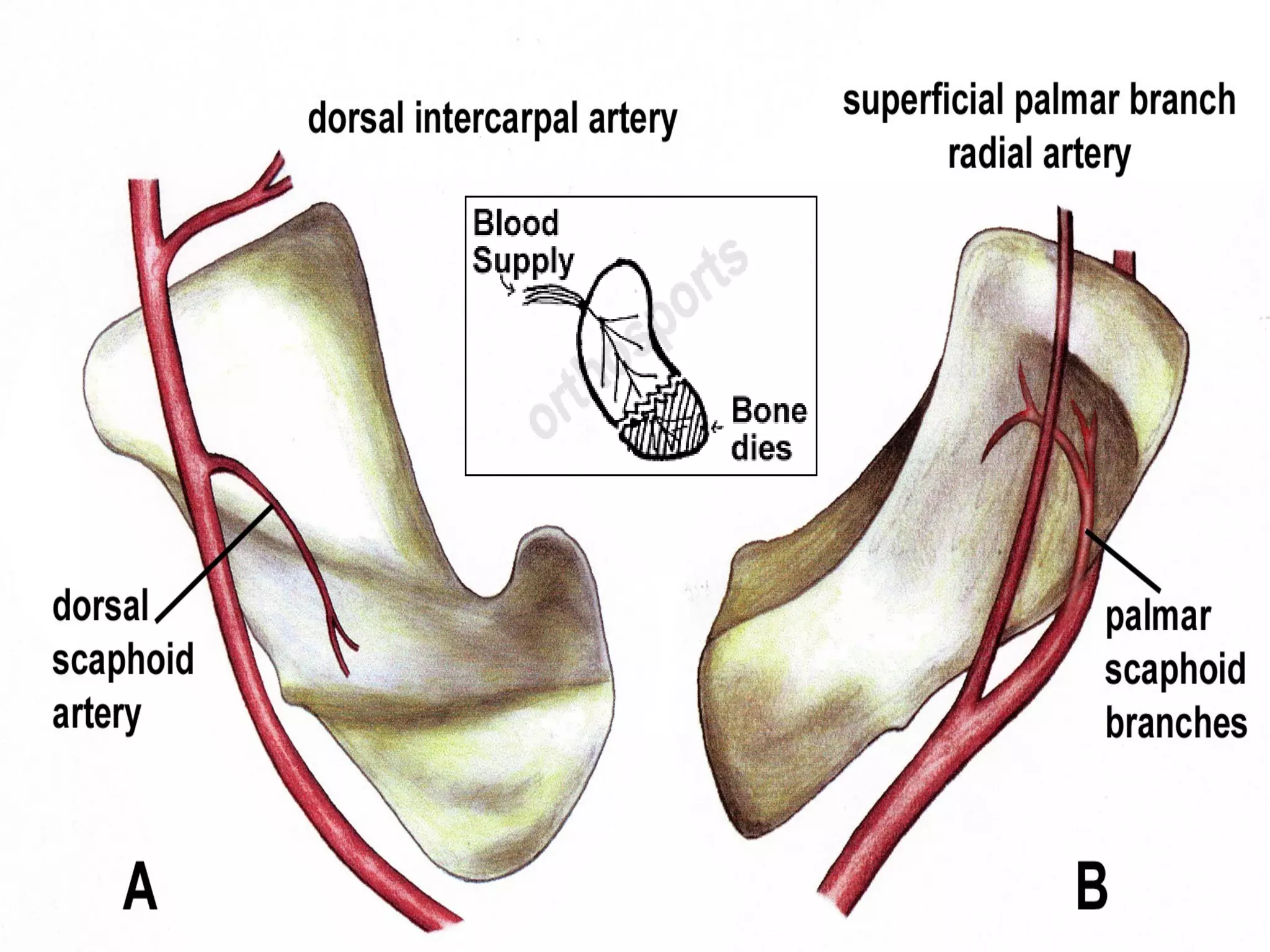
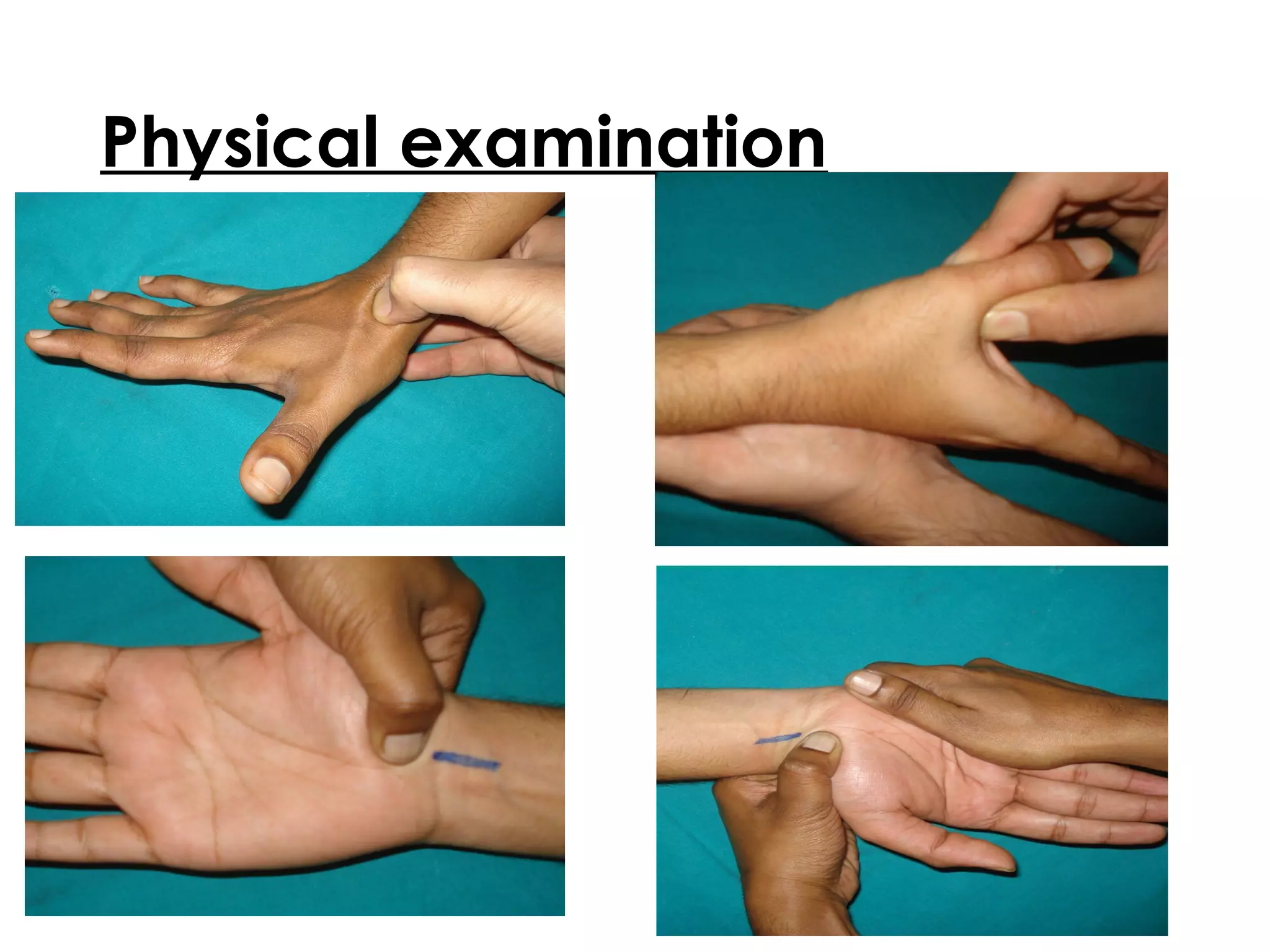
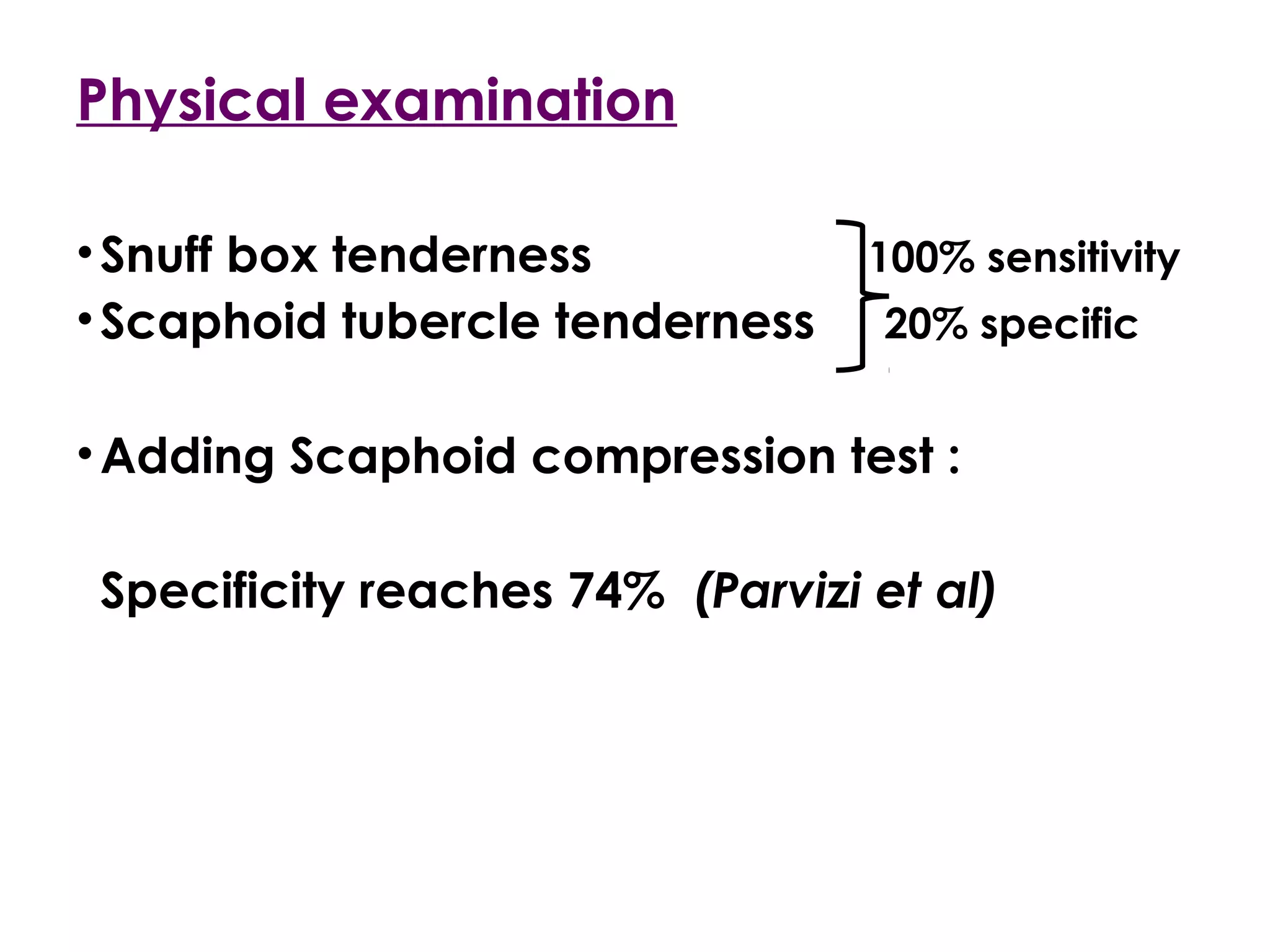
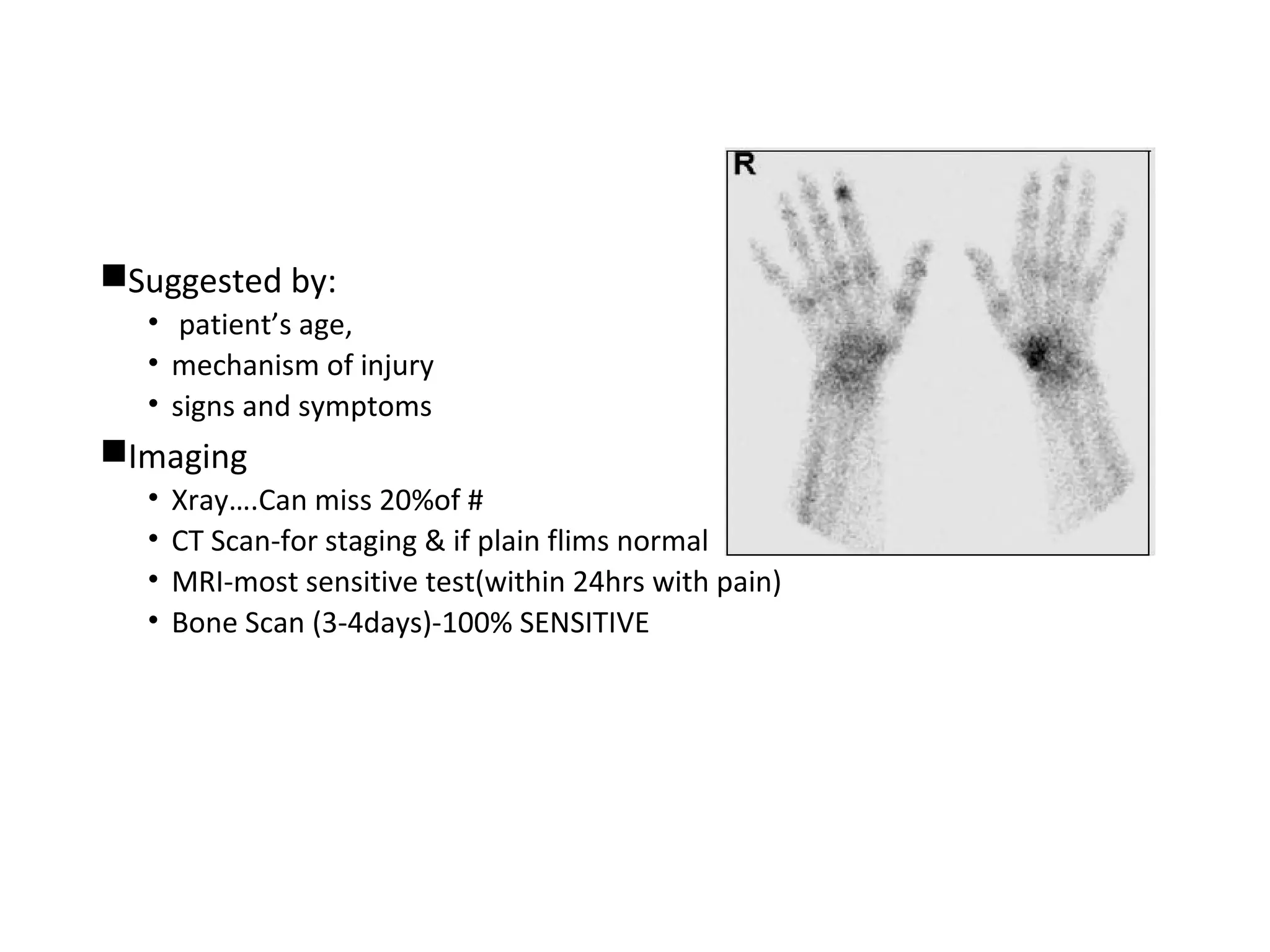


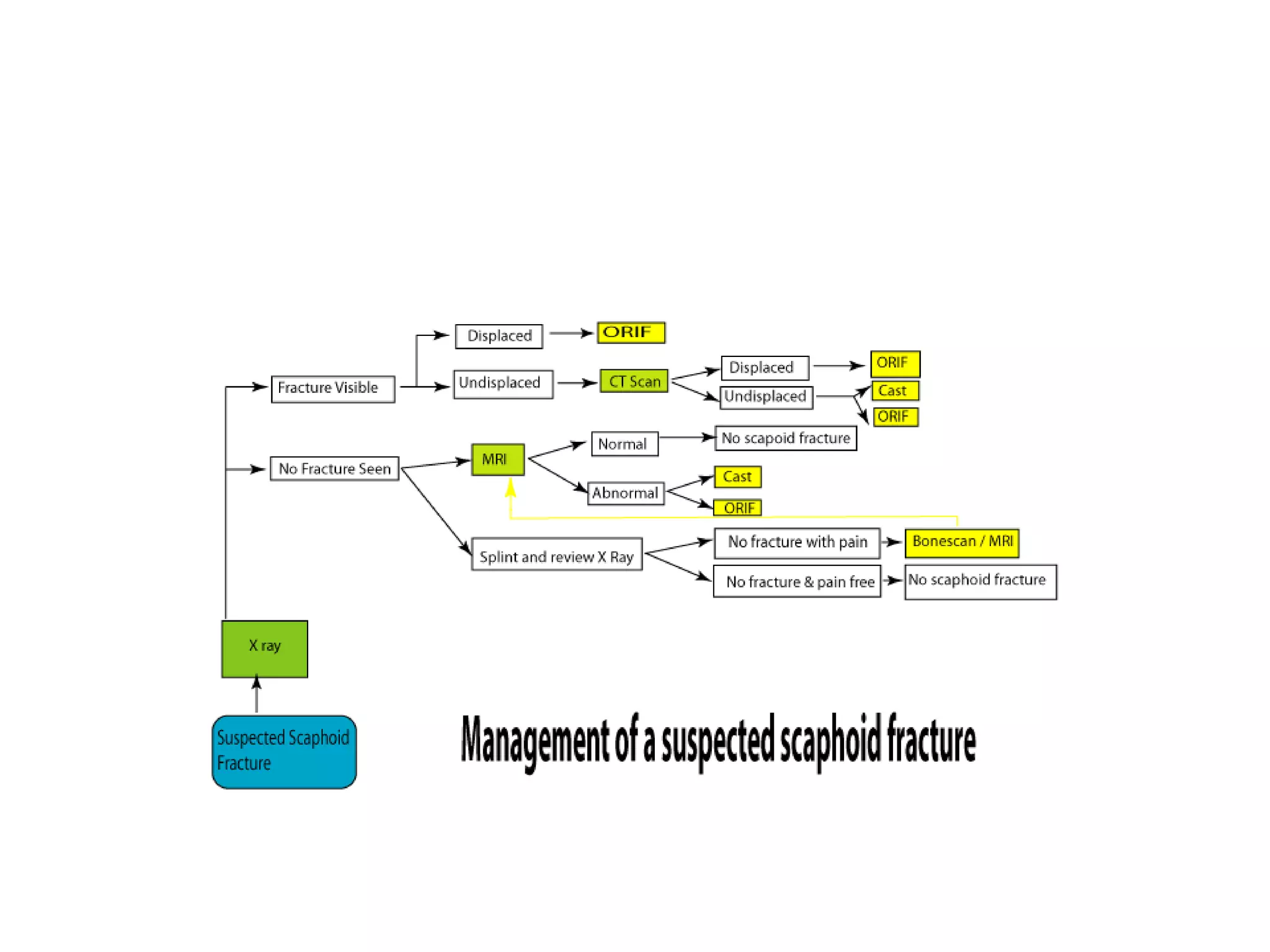
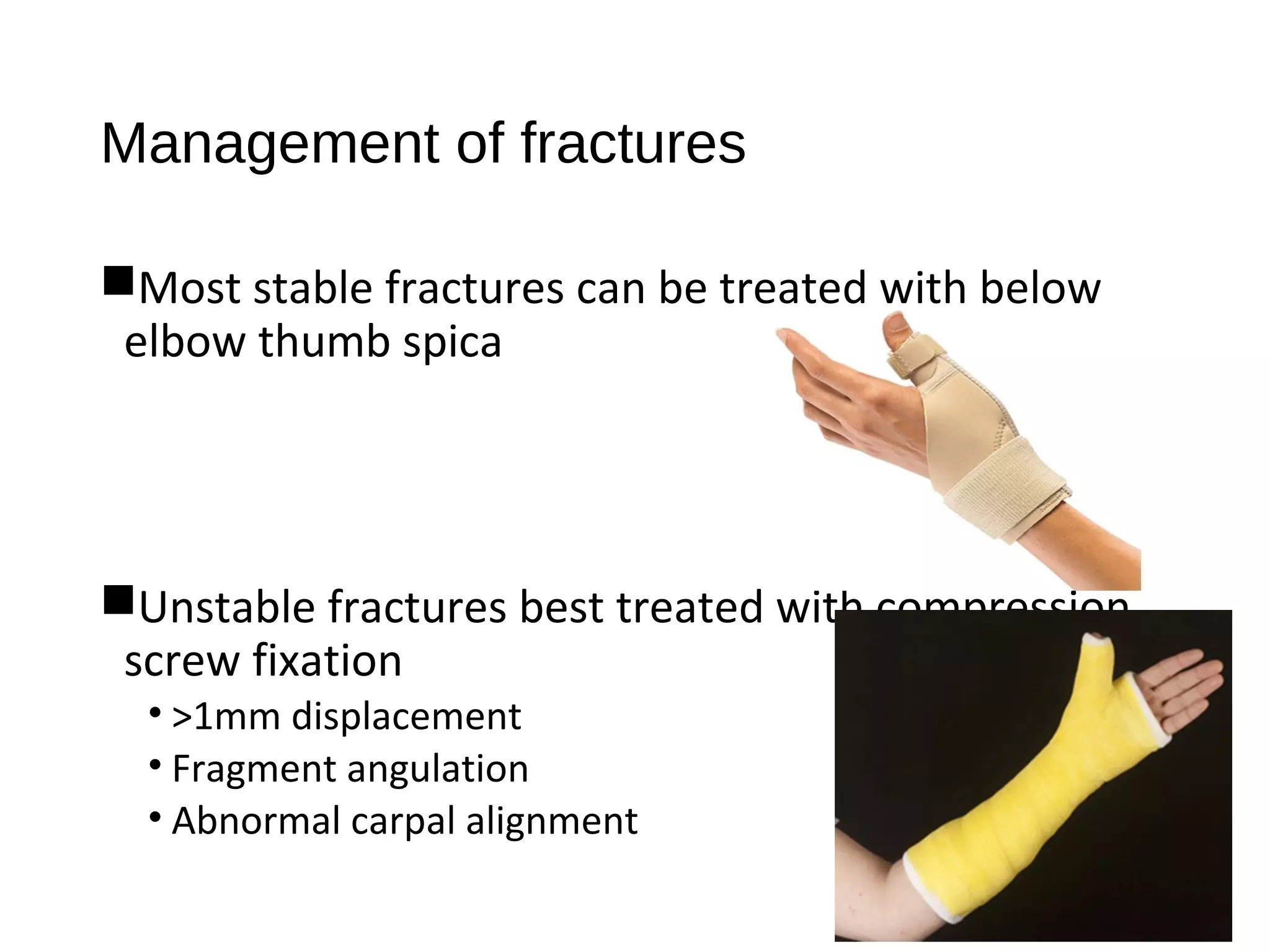






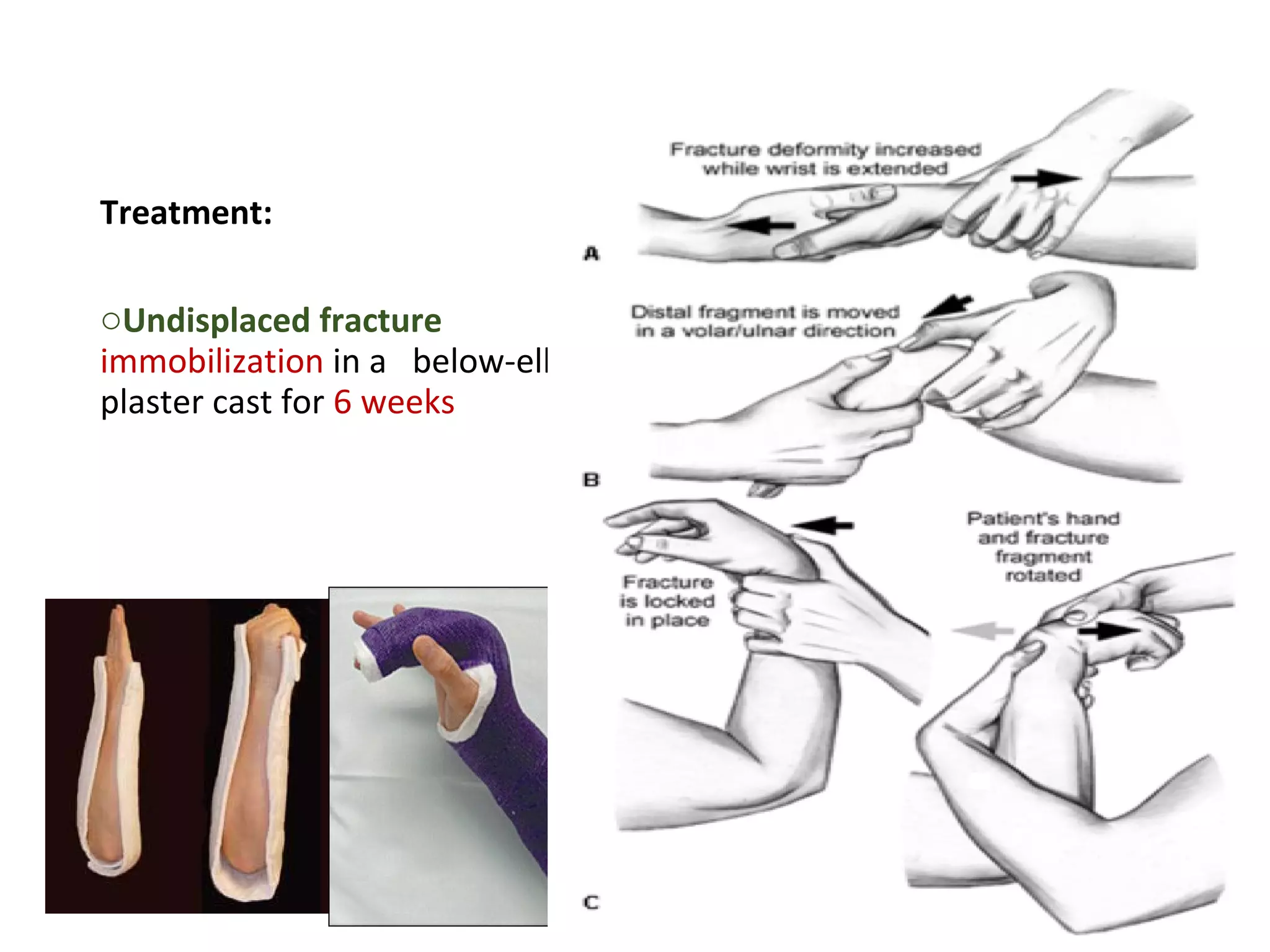


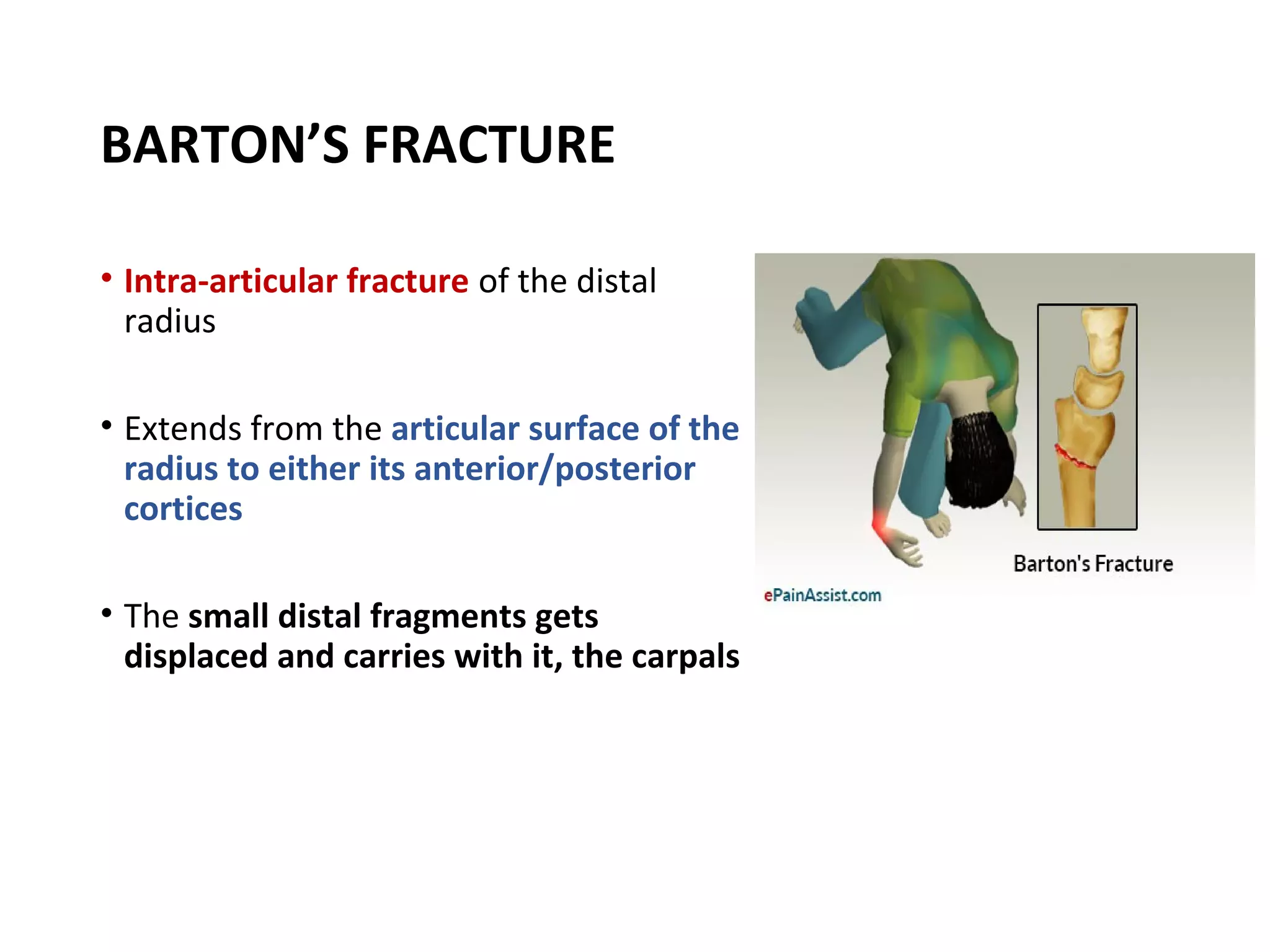

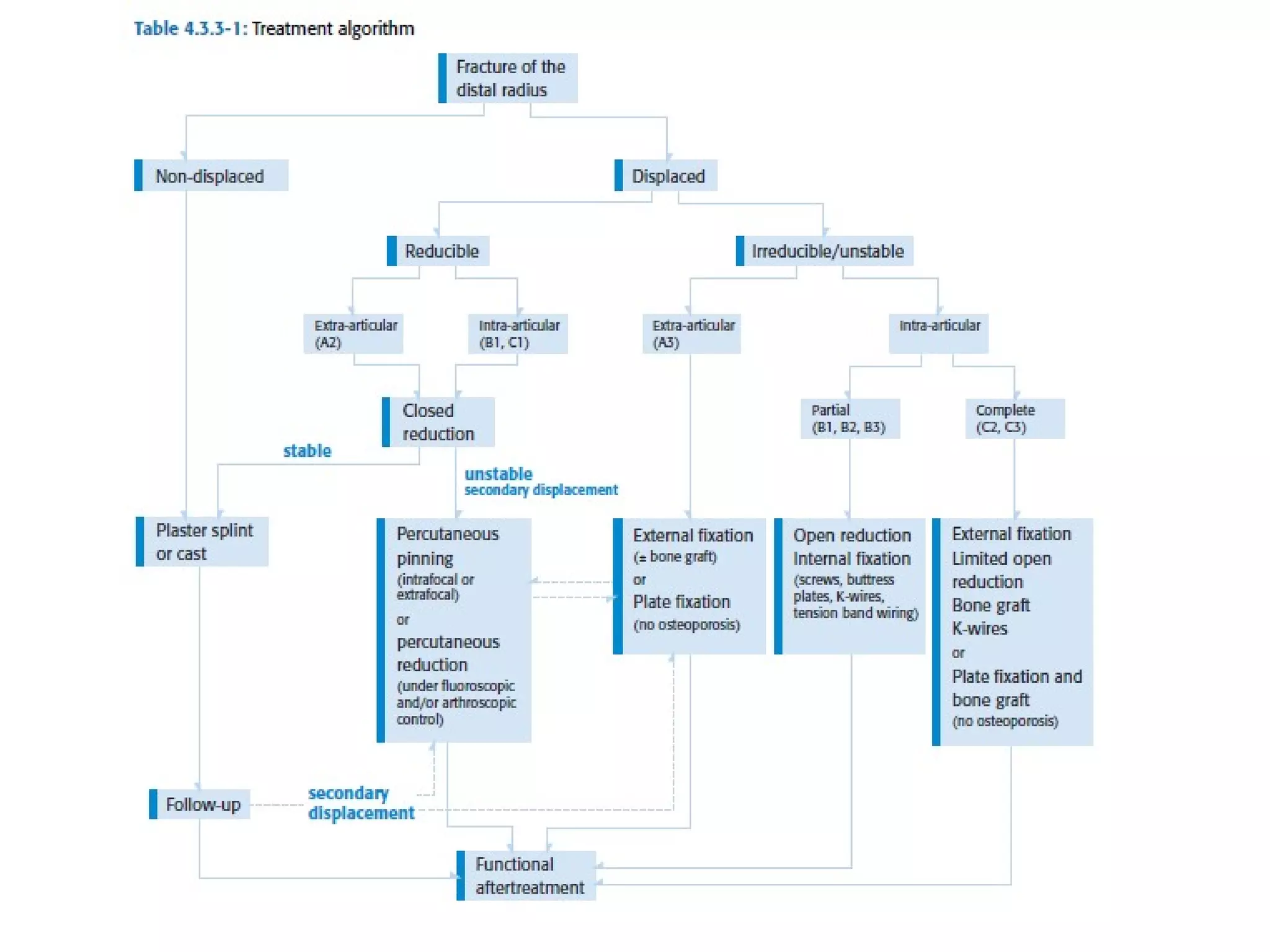







This document discusses various types of wrist fractures including scaphoid fractures, Colles' fractures, Smith's fractures, and Barton's fractures. Scaphoid fractures are the most common carpal bone fractures, often occurring in the waist or mid-portion from falls onto an outstretched hand. Physical examination findings and imaging can help diagnose these fractures. Treatment depends on fracture stability and displacement, ranging from splinting to screw fixation. Complications may include malunion or avascular necrosis.











































![FOREARM_FRACTURES[1].pptx and management](https://cdn.slidesharecdn.com/ss_thumbnails/forearmfractures1-250813120934-75e3f6d7-thumbnail.jpg?width=640&height=640&fit=bounds)






















![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)













