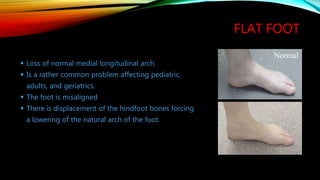
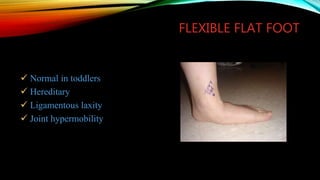
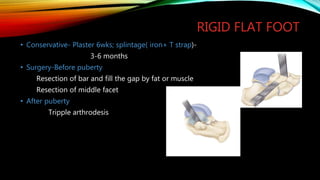
Flat foot, also known as pes planus, is a condition where the arch of the foot collapses, causing the entire sole of the foot to touch the ground. It can be congenital or acquired later in life. Flexible flat foot can be corrected by dorsiflexing the toes while rigid flat foot cannot. Treatment depends on the type and severity, ranging from exercises and orthotics to reconstructive surgery like triple arthrodesis for rigid flat foot. The goal is to relieve pain by restoring the arch alignment and motion of the foot.






































































![flat foot.ppt [pes planus ] #physio.# rehabilitation](https://cdn.slidesharecdn.com/ss_thumbnails/flatfoot-240310065759-517e9bef-thumbnail.jpg?width=640&height=640&fit=bounds)






































