Downloaded 65 times

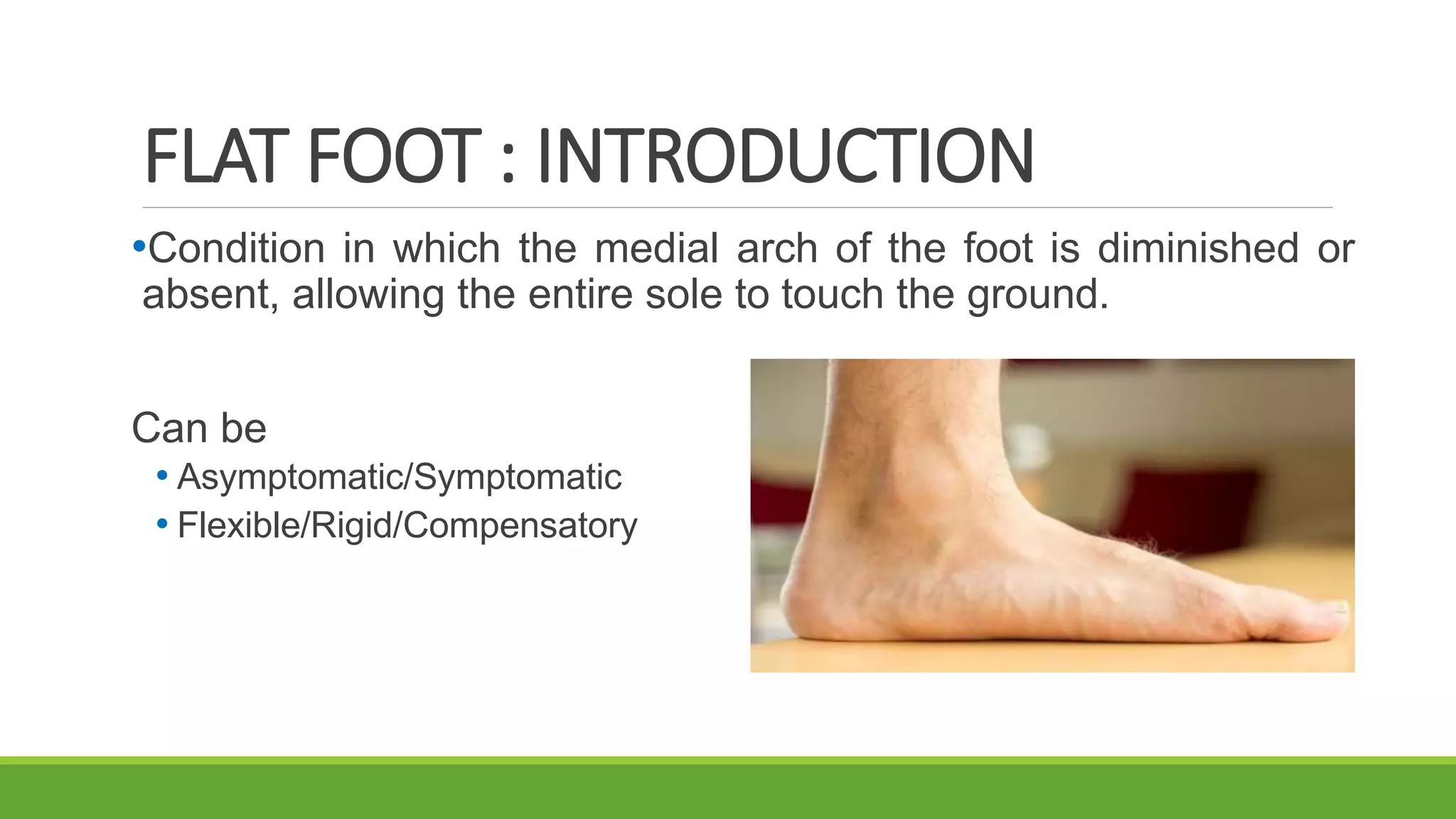

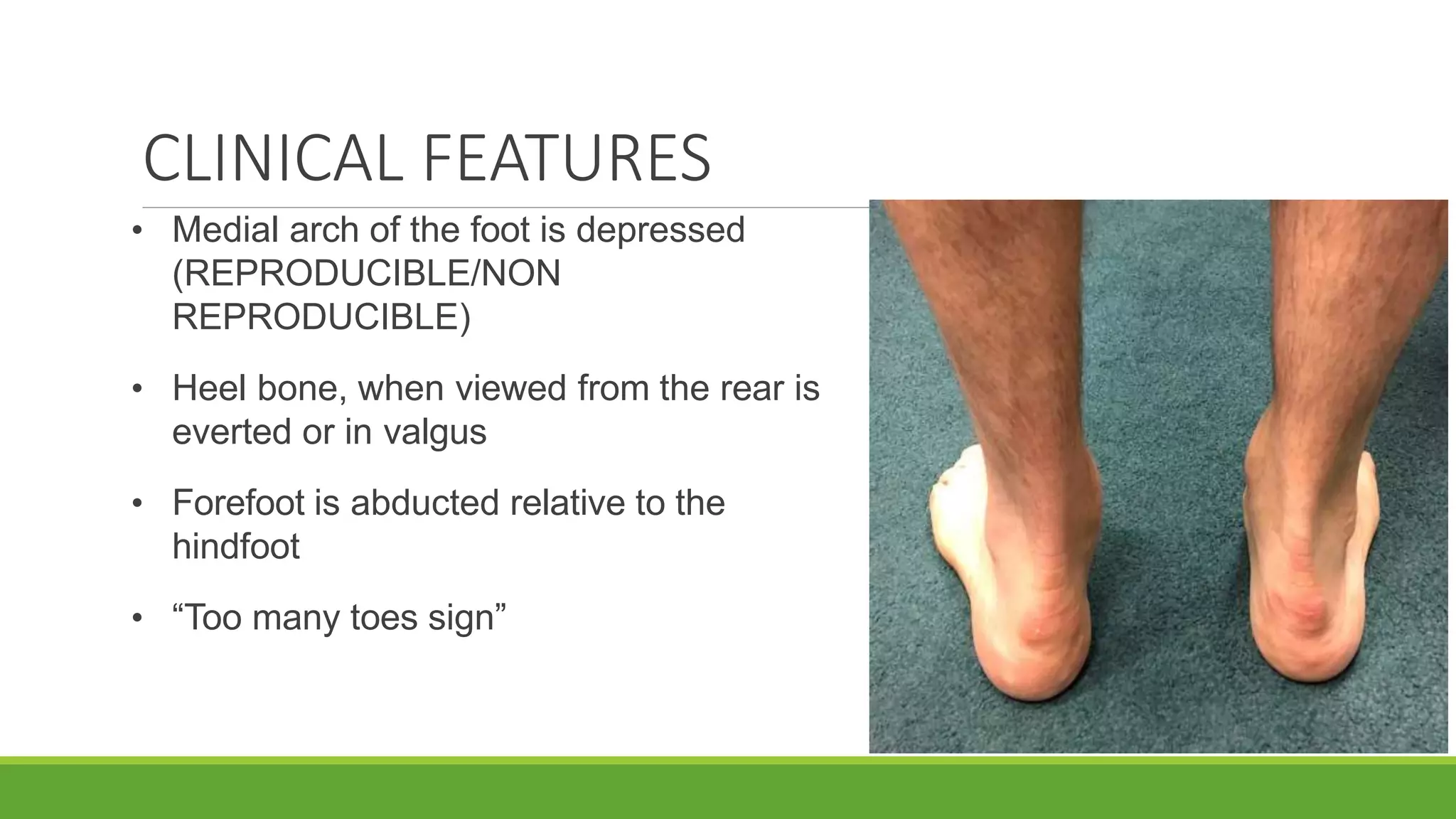
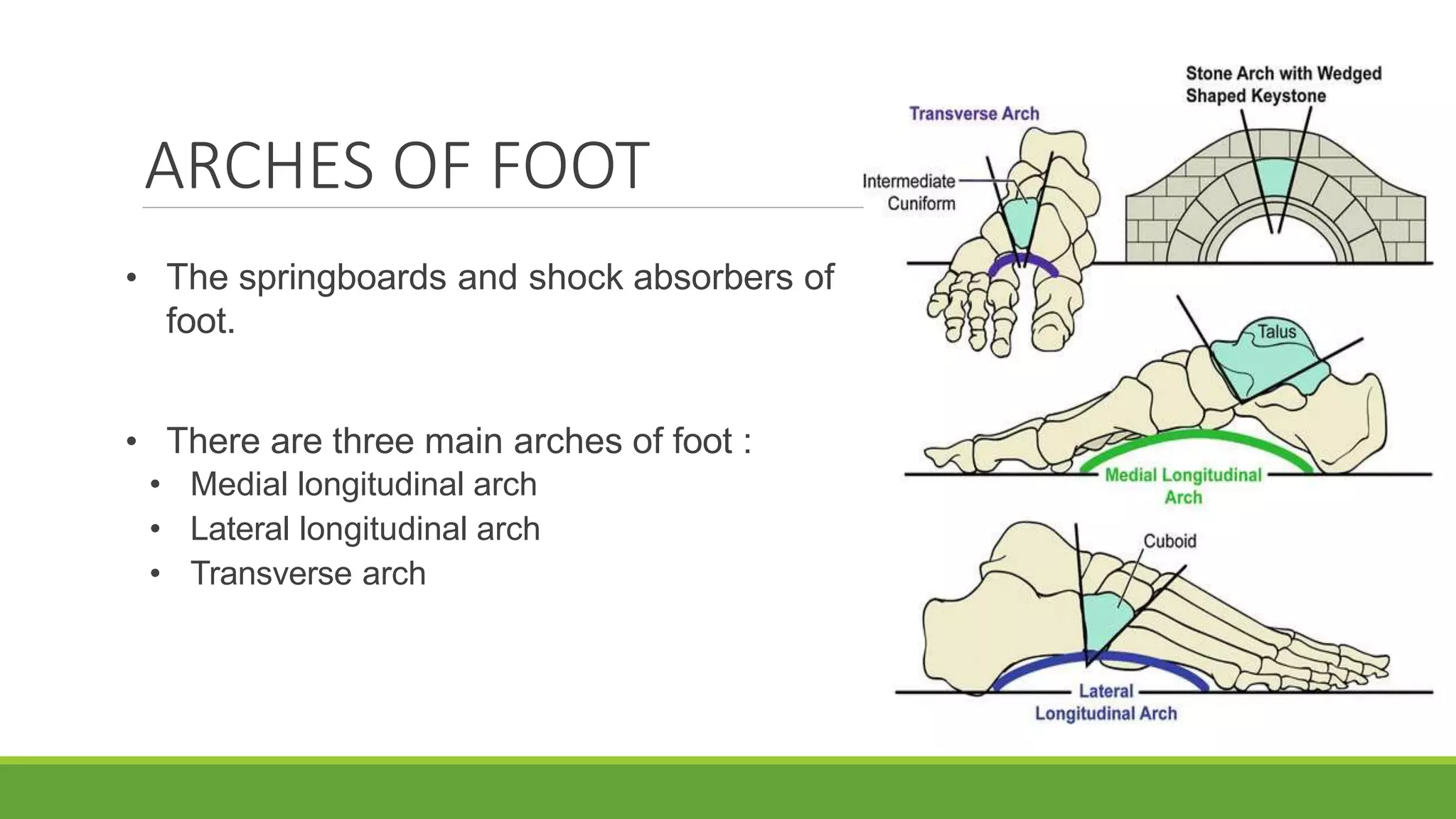

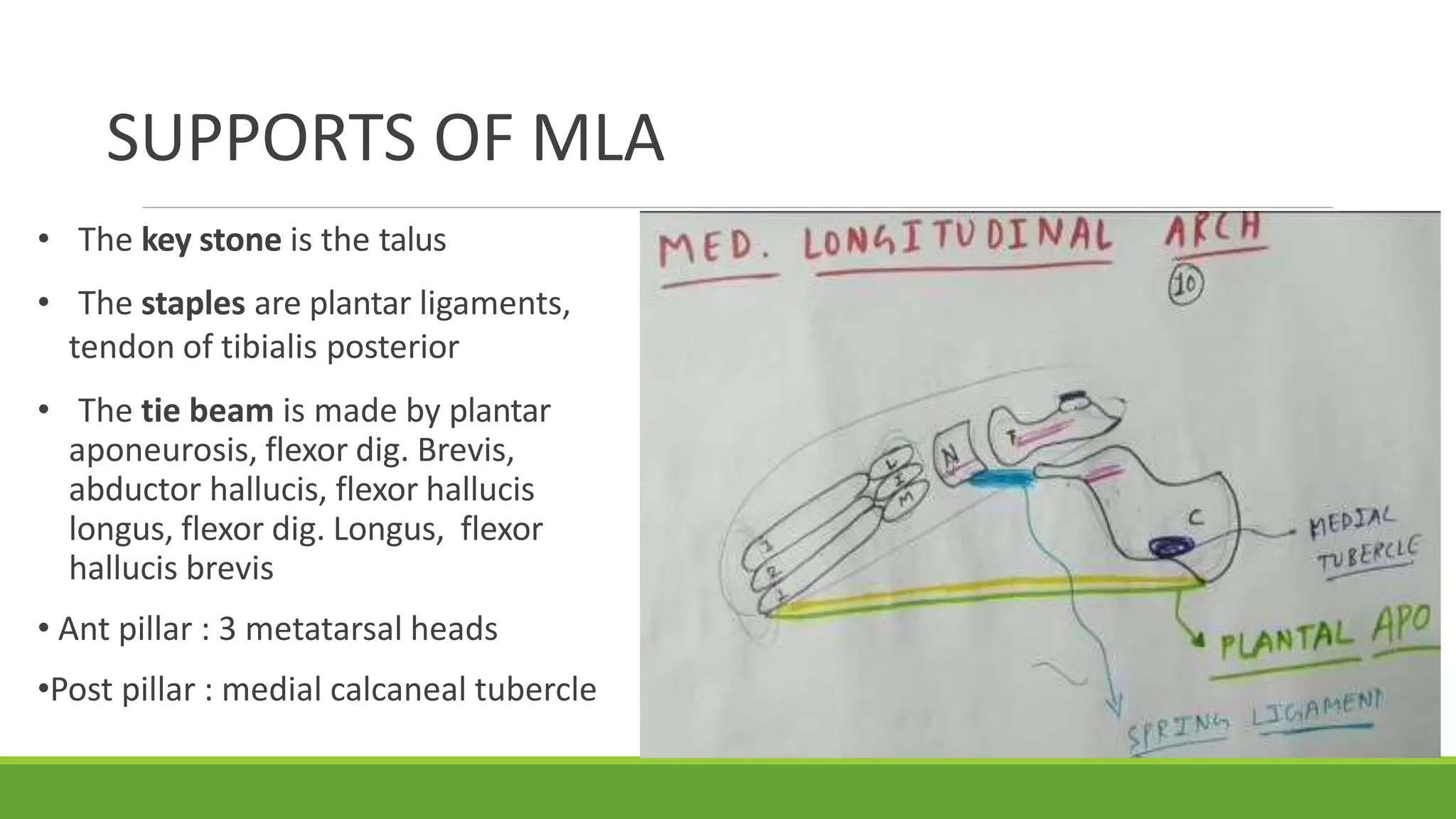
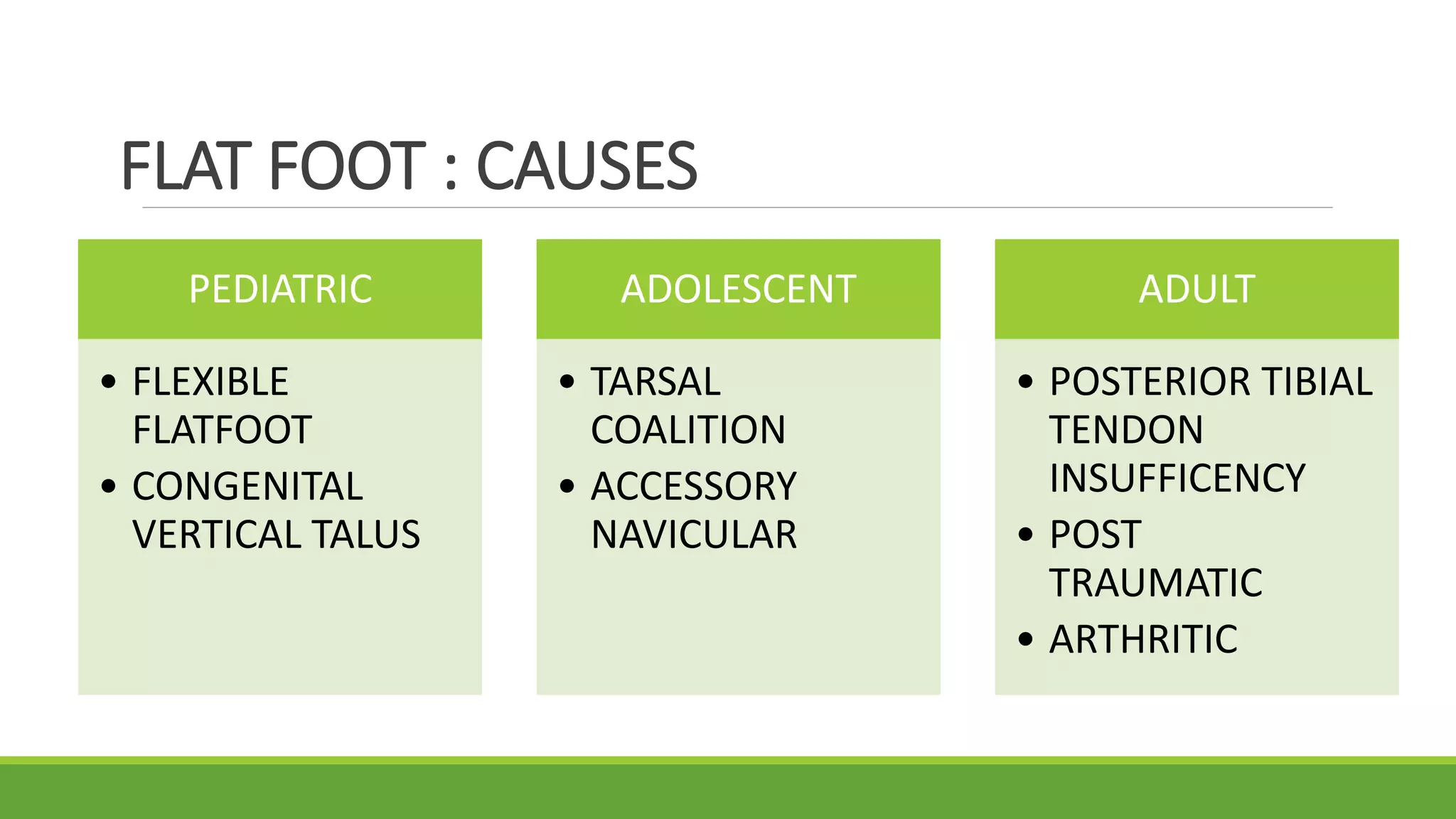

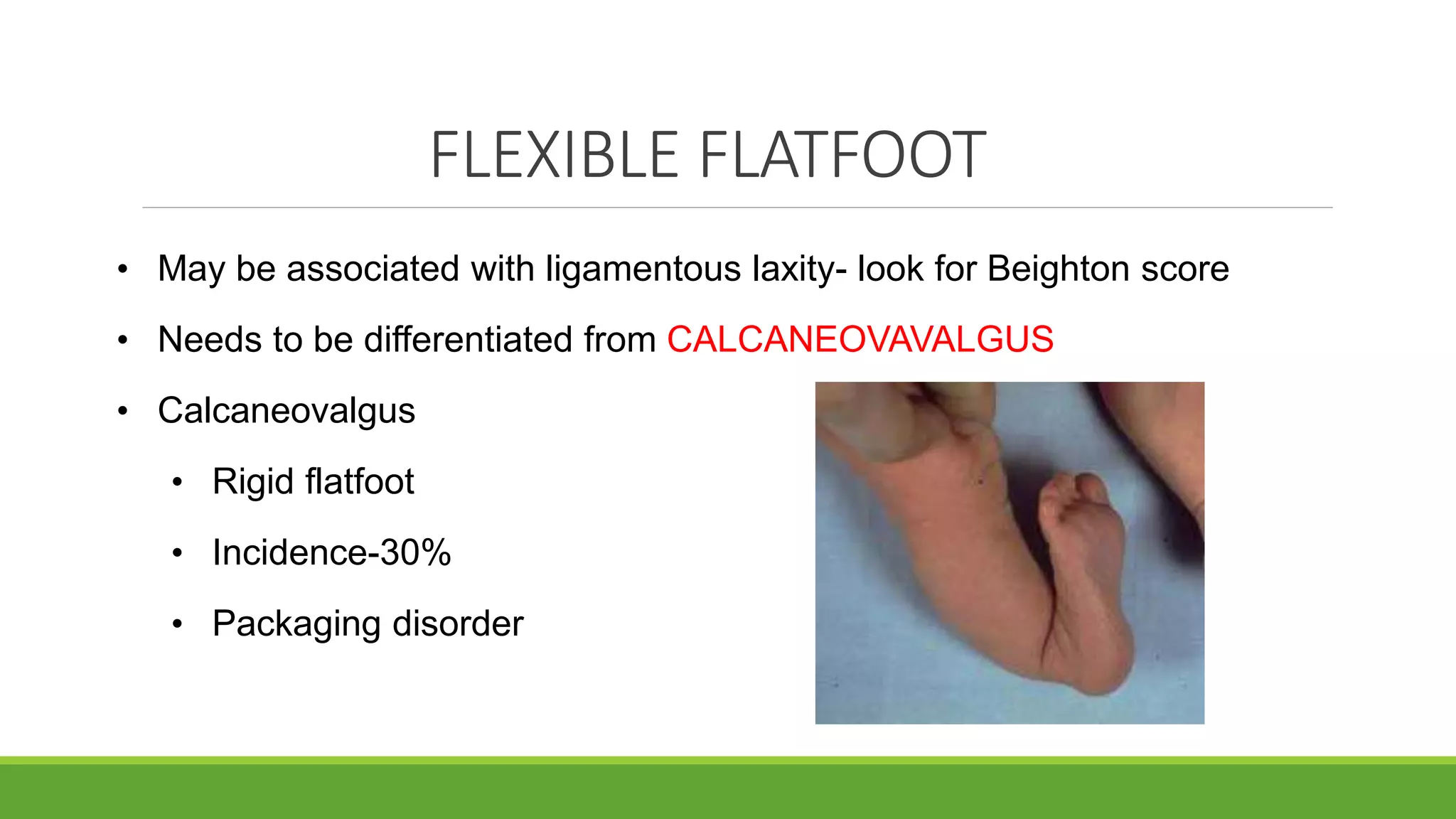
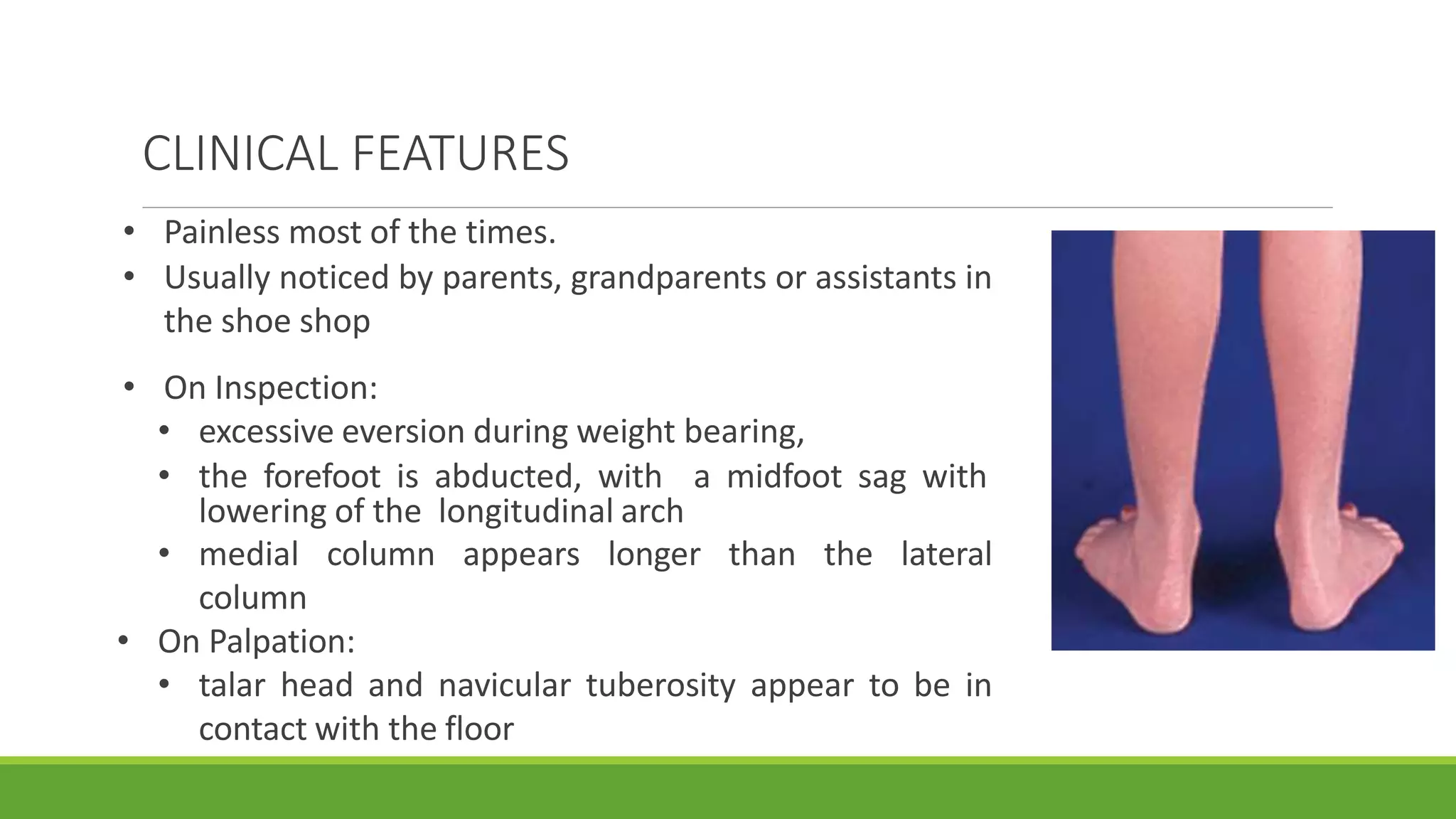
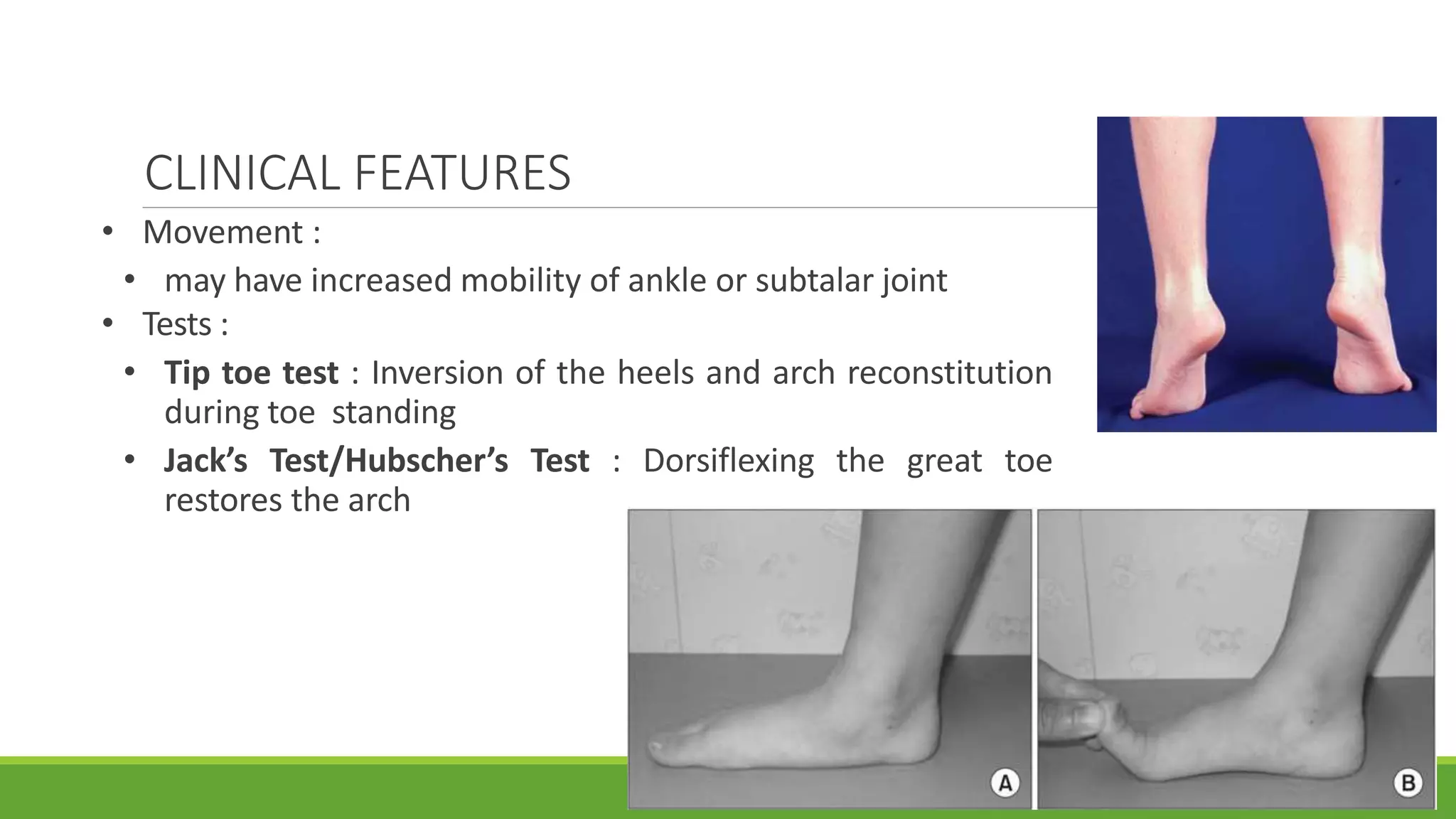



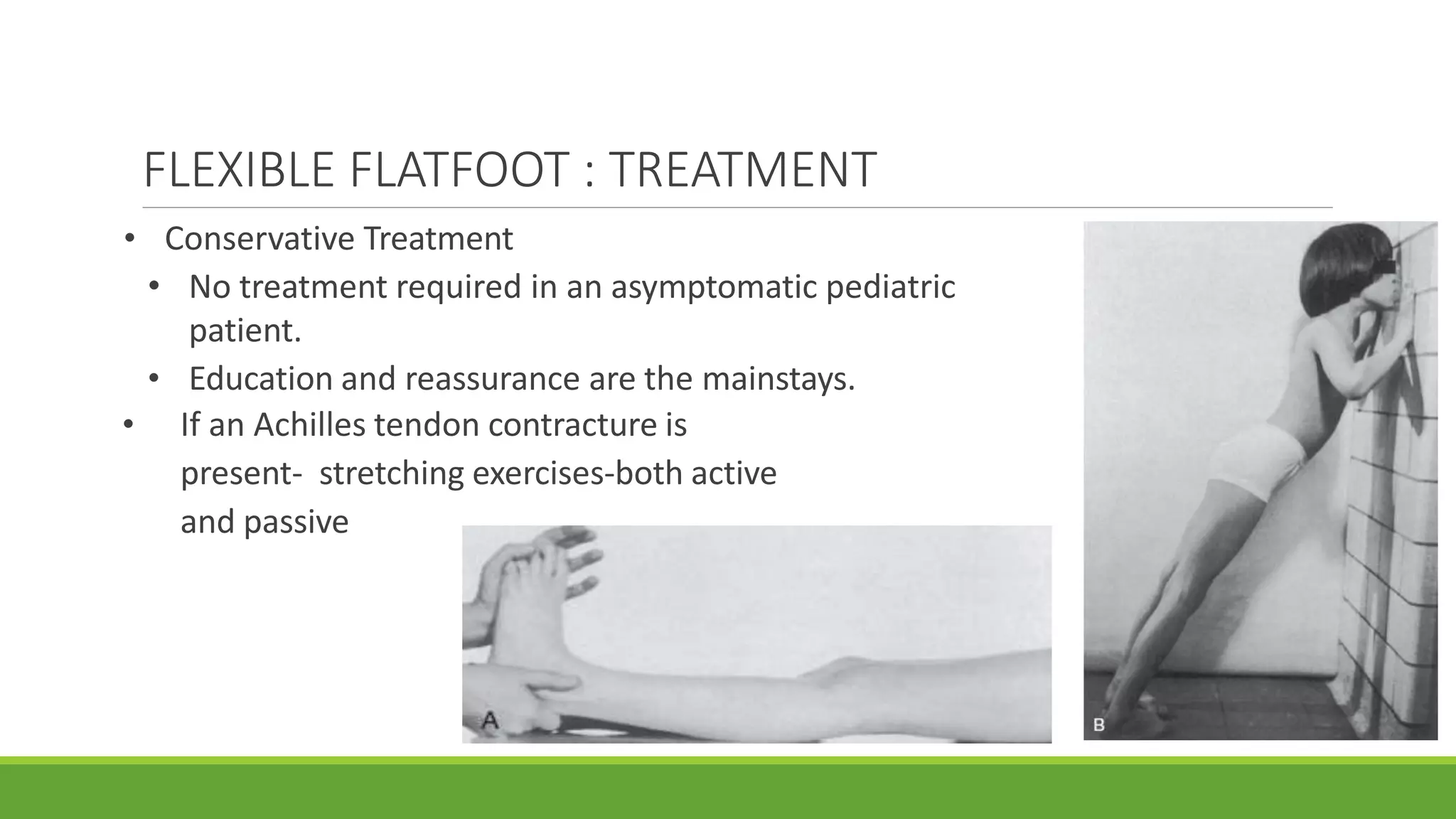
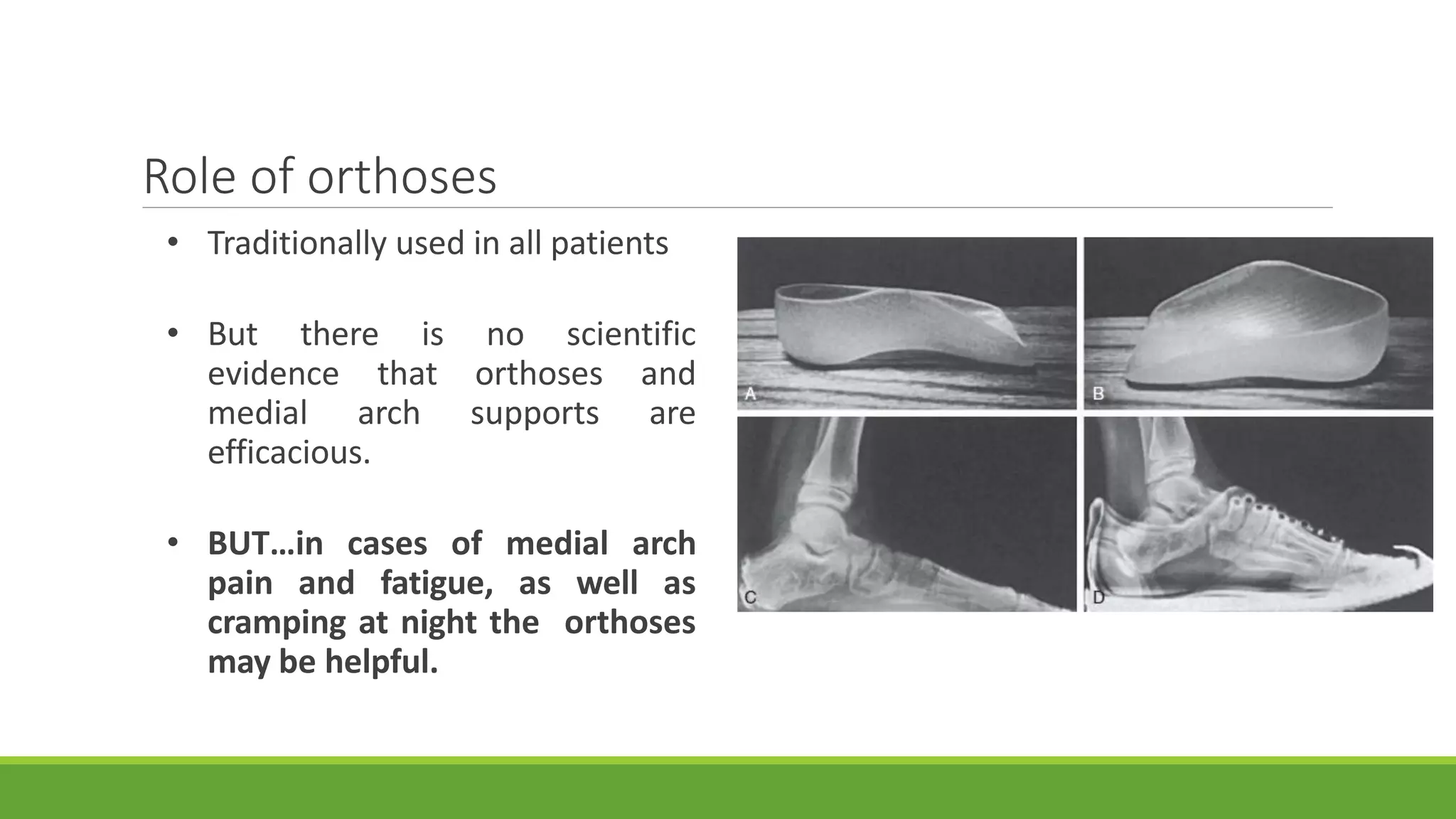
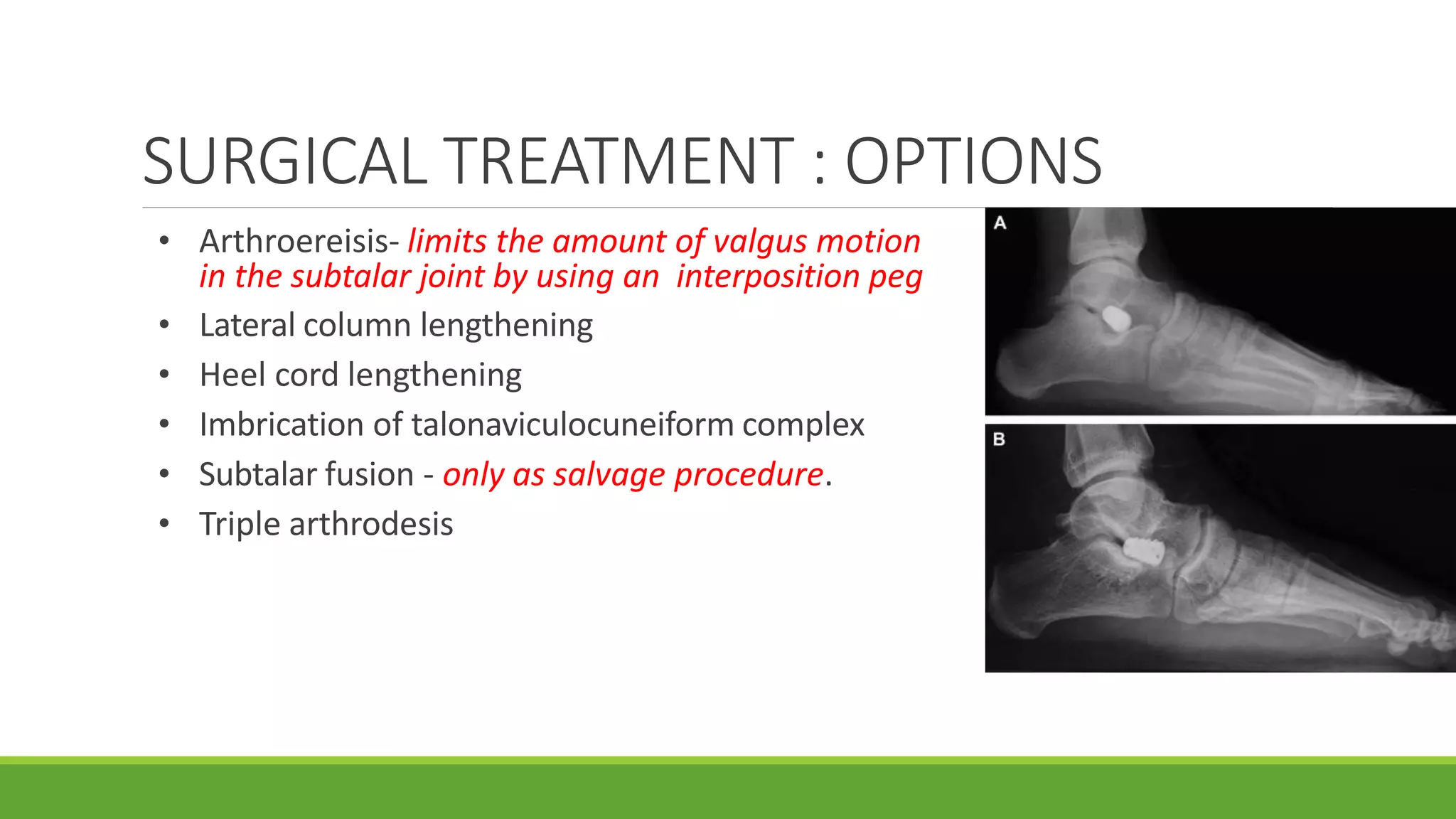

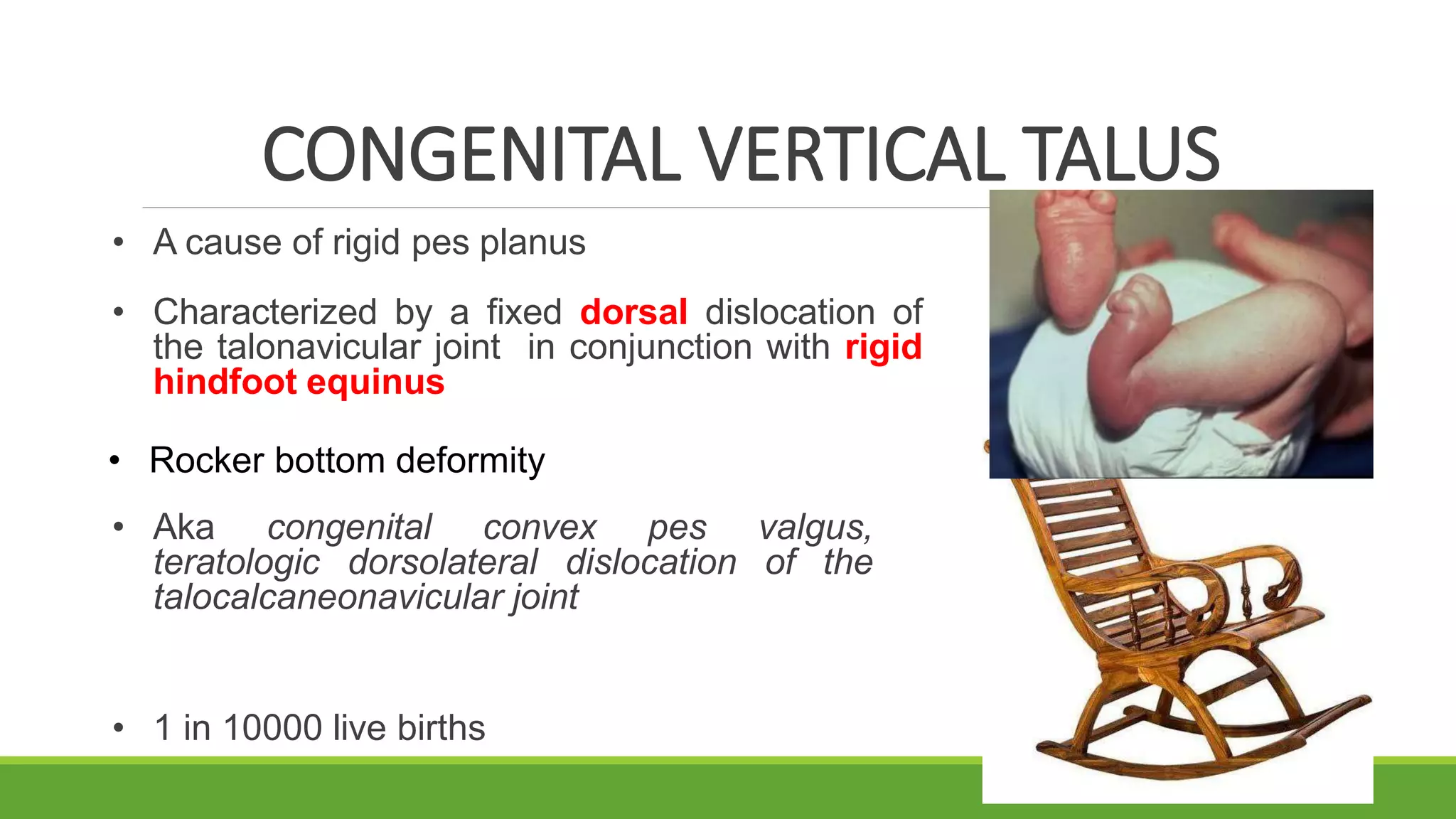


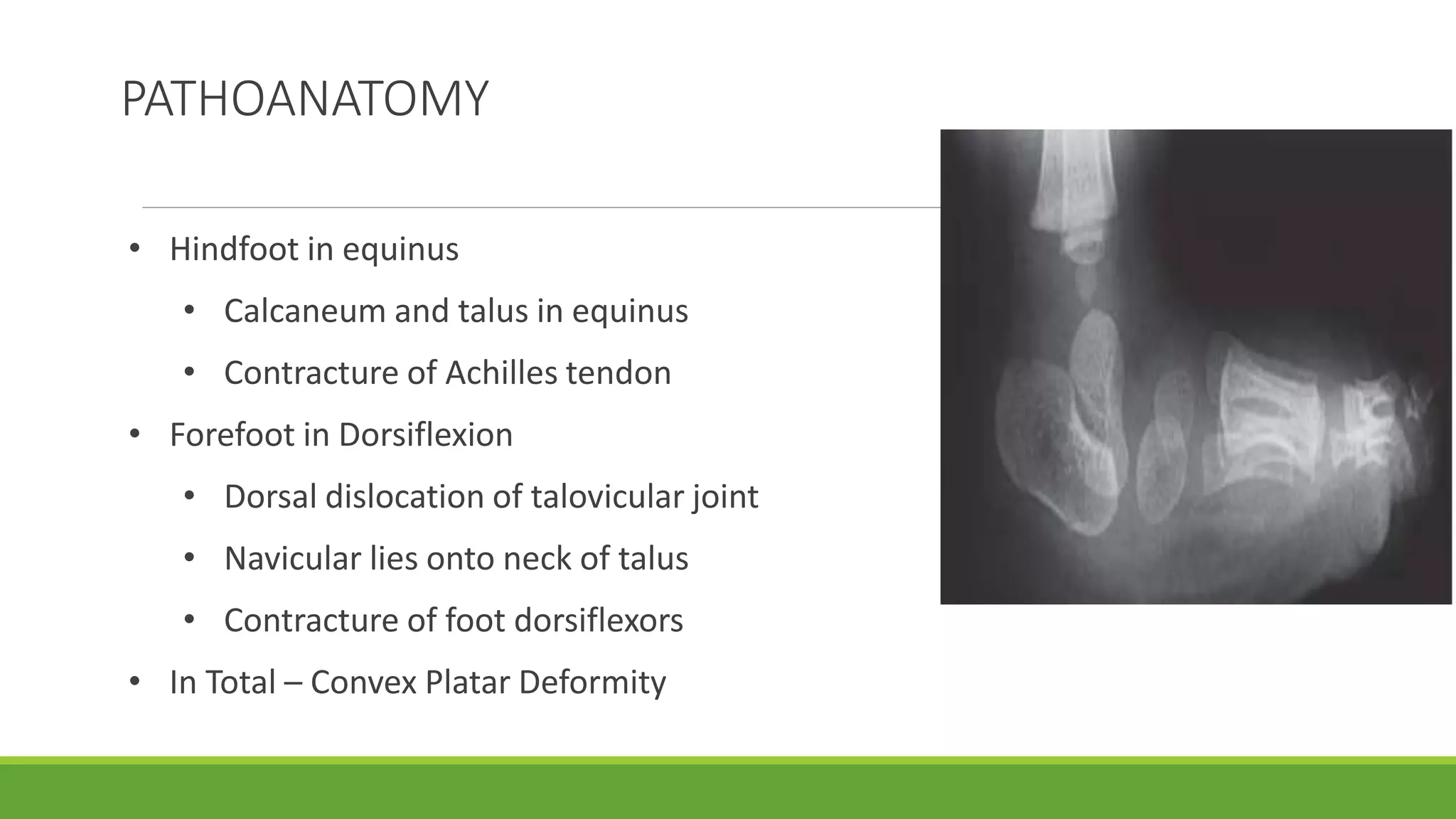




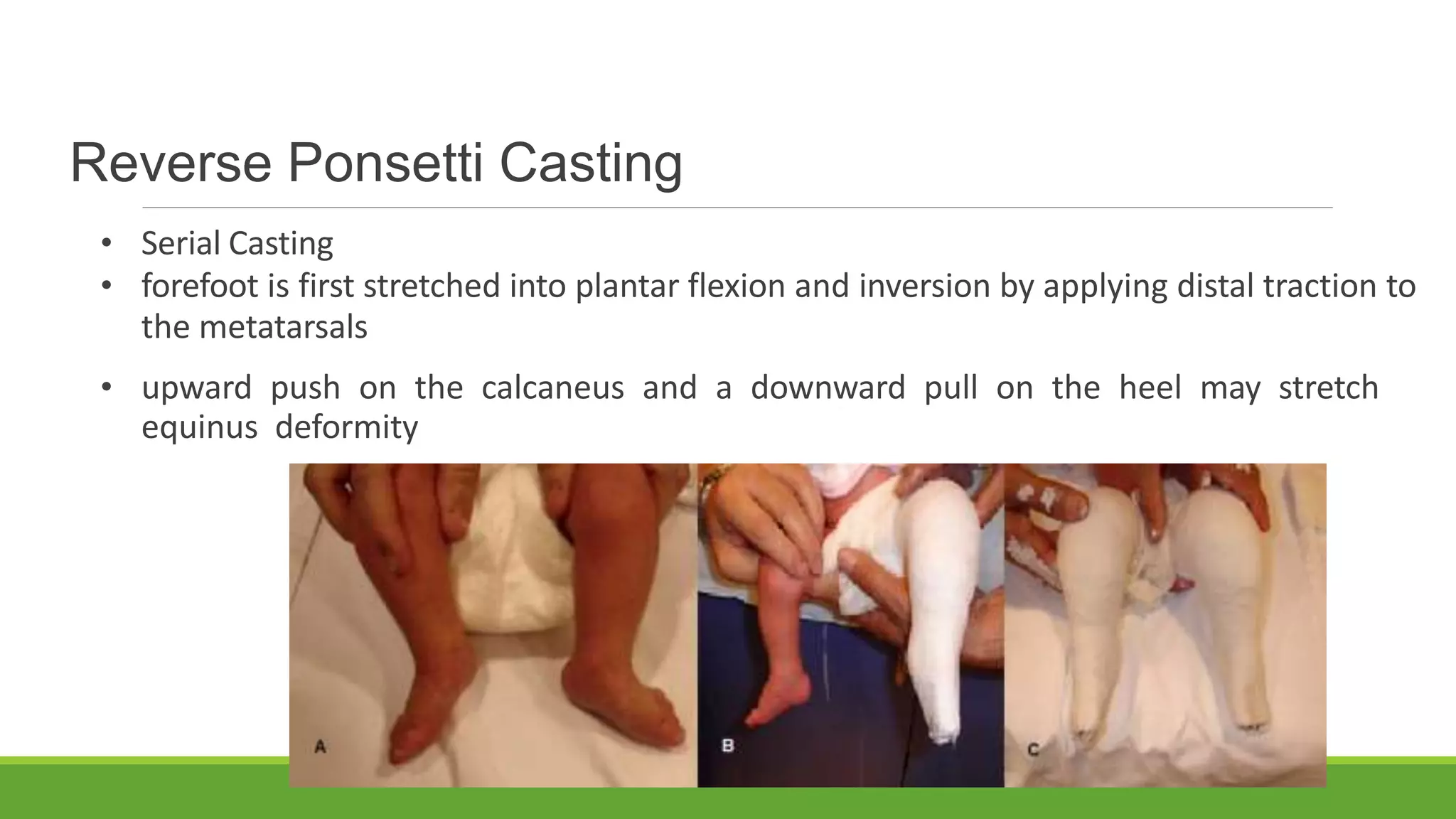




























This document discusses several foot conditions including pes planus (flat foot), pes valgus, flexible flat foot, congenital vertical talus, tarsal coalition, and posterior tibial tendon disorder. It provides details on the anatomy of the foot arches, clinical features, causes, treatments and imaging findings for each condition. Common causes of flat foot discussed include flexible flat foot in children, congenital vertical talus, tarsal coalition, and posterior tibial tendon insufficiency in adults. Imaging can help evaluate the degree of deformity and guide treatment, which may include orthotics, casting, or surgery depending on the condition.




































![flat foot.ppt [pes planus ] #physio.# rehabilitation](https://cdn.slidesharecdn.com/ss_thumbnails/flatfoot-240310065759-517e9bef-thumbnail.jpg?width=640&height=640&fit=bounds)








































