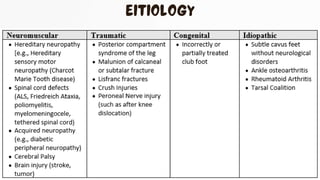
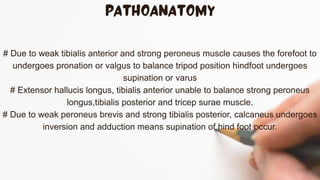
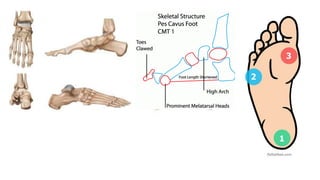
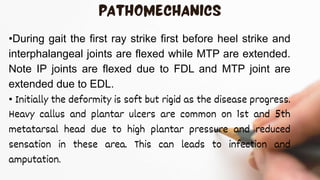
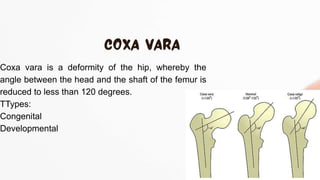
The document discusses various foot and hip deformities including pes cavus, pes planus, and coxa vara, outlining their characteristics, symptoms, and implications for gait and pressure distribution. It describes the causes and treatment options, including physical therapy, orthotic support, and surgical interventions, emphasizing the importance of balancing treatment for both pain relief and functional mobility. Data on demographics, physical examination methods, and rehabilitation strategies are provided to guide assessment and management of these conditions.























![flat foot.ppt [pes planus ] #physio.# rehabilitation](https://cdn.slidesharecdn.com/ss_thumbnails/flatfoot-240310065759-517e9bef-thumbnail.jpg?width=640&height=640&fit=bounds)



































